Saffari Tiam M, Bedar Meiwand, Hundepool Caroline A, Bishop Allen T, Shin Alexander Y
Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN, USA; Department of Plastic, Reconstructive and Hand Surgery, Erasmus Medical Center, Rotterdam, the Netherlands.
Department of Plastic, Reconstructive and Hand Surgery, Erasmus Medical Center, Rotterdam, the Netherlands.
Neural Regen Res. 2020 Sep;15(9):1573-1579. doi: 10.4103/1673-5374.276327.
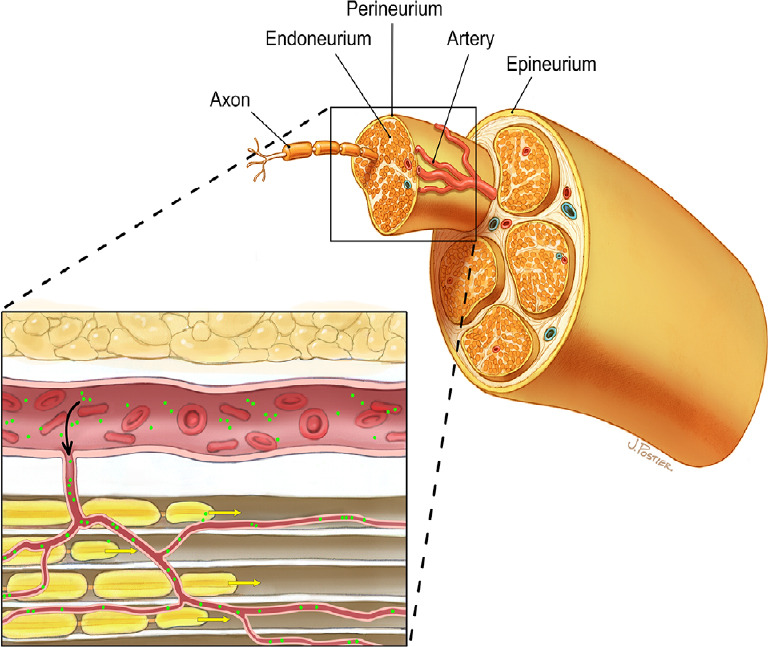
Vascularization is an important factor in nerve graft survival and function. The specific molecular regulations and patterns of angiogenesis following peripheral nerve injury are in a broad complex of pathways. This review aims to summarize current knowledge on the role of vascularization in nerve regeneration, including the key regulation molecules, and mechanisms and patterns of revascularization after nerve injury. Angiogenesis, the maturation of pre-existing vessels into new areas, is stimulated through angiogenic factors such as vascular endothelial growth factor and precedes the repair of damaged nerves. Vascular endothelial growth factor administration to nerves has demonstrated to increase revascularization after injury in basic science research. In the clinical setting, vascularized nerve grafts could be used in the reconstruction of large segmental peripheral nerve injuries. Vascularized nerve grafts are postulated to accelerate revascularization and enhance nerve regeneration by providing an optimal nutritional environment, especially in scarred beds, and decrease fibroblast infiltration. This could improve functional recovery after nerve grafting, however, conclusive evidence of the superiority of vascularized nerve grafts is lacking in human studies. A well-designed randomized controlled trial comparing vascularized nerve grafts to non-vascularized nerve grafts involving patients with similar injuries, nerve graft repair and follow-up times is necessary to demonstrate the efficacy of vascularized nerve grafts. Due to technical challenges, composite transfer of a nerve graft along with its adipose tissue has been proposed to provide a healthy tissue bed. Basic science research has shown that a vascularized fascial flap containing adipose tissue and a vascular bundle improves revascularization through excreted angiogenic factors, provided by the stem cells in the adipose tissue as well as by the blood supply and environmental support. While it was previously believed that revascularization occurred from both nerve ends, recent studies propose that revascularization occurs primarily from the proximal nerve coaptation. Fascial flaps or vascularized nerve grafts have limited applicability and future directions could lead towards off-the-shelf alternatives to autografting, such as biodegradable nerve scaffolds which include capillary-like networks to enable vascularization and avoid graft necrosis and ischemia.
血管化是神经移植存活和功能的重要因素。周围神经损伤后血管生成的具体分子调控和模式涉及广泛复杂的信号通路。本综述旨在总结当前关于血管化在神经再生中作用的知识,包括关键调控分子以及神经损伤后血管再形成的机制和模式。血管生成是指已有血管向新区域的成熟过程,通过血管内皮生长因子等血管生成因子刺激,先于受损神经的修复。在基础科学研究中,向神经施用血管内皮生长因子已证明可增加损伤后的血管再形成。在临床环境中,带血管神经移植可用于大段周围神经损伤的重建。带血管神经移植被认为可通过提供最佳营养环境来加速血管再形成并增强神经再生,尤其是在瘢痕化床中,并减少成纤维细胞浸润。这可能会改善神经移植后的功能恢复,然而,在人体研究中缺乏带血管神经移植优越性的确凿证据。需要进行一项精心设计的随机对照试验,比较带血管神经移植与非带血管神经移植对具有相似损伤、神经移植修复和随访时间的患者的效果,以证明带血管神经移植的疗效。由于技术挑战,已提出将神经移植与其脂肪组织进行复合移植以提供健康的组织床。基础科学研究表明,包含脂肪组织和血管束的带血管筋膜瓣可通过脂肪组织中的干细胞分泌的血管生成因子以及血液供应和环境支持来改善血管再形成。虽然以前认为血管再形成从神经两端发生,但最近的研究提出血管再形成主要从近端神经吻合处发生。筋膜瓣或带血管神经移植的适用性有限,未来的方向可能是开发现成的自体移植替代物,如可生物降解的神经支架,其包括毛细血管样网络以实现血管化并避免移植坏死和缺血。