Service de Réanimation Néonatale et Néonatalogie, Hôpital Delafontaine, 2 rue Dr Delafontaine, 93205, Saint-Denis, France.
Unité de Recherche Clinique, Groupe Hospitalier Paris Seine Saint-Denis, APHP, Bobigny, France.
BMC Pediatr. 2020 Apr 1;20(1):144. doi: 10.1186/s12887-020-02055-3.
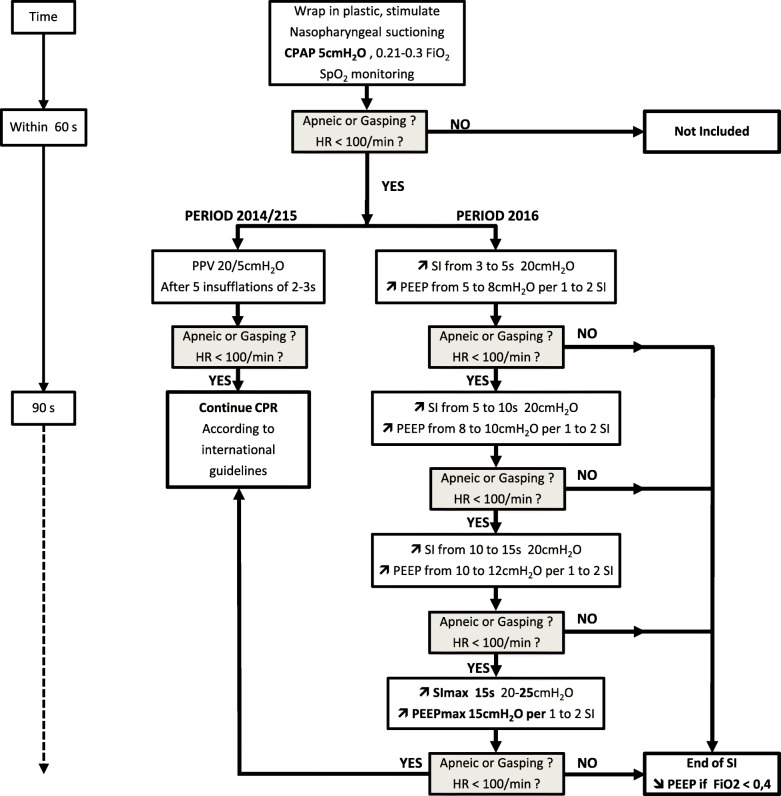
Lung recruitment at birth has been advocated as an effective method of improving the respiratory transition at birth. Sustained inflations (SI) and dynamic positive end-expiratory pressure (PEEP) were assessed in clinical and animal studies to define the optimal level. Our working hypothesis was that very low gestational age infants (VLGAI) < 32 weeks' gestation require an individualized lung recruitment based on combining both manoeuvers.
Between 2014 and 2016, 91 and 72 inborn VLGAI, requiring a respiratory support beyond a continuous positive airway pressure (CPAP) = 5 cmH2O, were enrolled before and after introducing these manoeuvers based on progressive increase in SI up to 15 s, with simultaneous gradual increase in PEEP up to 15 cmH2O, according to the cardiorespiratory response. Retrospective comparisons of the incidence of mechanical ventilation (MV) < 72 h of life, short-term and before discharge morbidity were then performed.
Among extremely low gestational age infants (ELGAI) < 29 weeks' gestation, the following outcomes decreased significantly: intubation (90 to 55%) and surfactant administration (54 to 12%) in the delivery room, MV (92 to 71%) and its mean duration < 72 h of life (45 h to 13 h), administration of a 2nd dose of surfactant (35 to 12%) and postnatal corticosteroids (52 to 19%), and the rate of bronchopulmonary dysplasia (23 to 5%). Among VLGAI, all of these results were also significant. Neonatal mortality and morbidity were not different.
In our setting, combining two individualized lung recruitment maneuvers at birth was feasible and may be beneficial on short-term and before discharge pulmonary outcomes. A randomized controlled trial is needed to confirm these results.
在出生时进行肺复张已被提倡为改善出生时呼吸过渡的有效方法。在临床和动物研究中评估了持续充气(SI)和动态呼气末正压(PEEP),以确定最佳水平。我们的工作假设是,极早产儿(VLGAI)<32 周妊娠需要基于联合两种操作的个体化肺复张。
在 2014 年至 2016 年期间,在引入这些操作之前和之后,根据 SI 逐渐增加至 15 秒,同时根据心肺反应逐渐增加 PEEP 至 15 cmH2O,纳入了 91 名和 72 名需要持续气道正压通气(CPAP)>5 cmH2O 以上呼吸支持的内在 VLGAI。根据心肺反应,逐渐增加 SI 至 15 秒,同时逐渐增加 PEEP 至 15 cmH2O。然后进行了机械通气(MV)<72 小时的发生率、短期和出院前发病率的回顾性比较。
在极早产儿(ELGAI)<29 周妊娠中,以下结果显著降低:分娩室中的插管(90%至 55%)和表面活性剂的使用(54%至 12%)、MV(92%至 71%)及其<72 小时的平均持续时间(45 小时至 13 小时)、第 2 次表面活性剂的给药(35%至 12%)和产后皮质类固醇(52%至 19%),以及支气管肺发育不良(BPD)的发生率(23%至 5%)。在 VLGAI 中,所有这些结果也都是显著的。新生儿死亡率和发病率没有差异。
在我们的环境中,在出生时联合使用两种个体化的肺复张操作是可行的,可能对短期和出院前的肺部结果有益。需要进行随机对照试验来证实这些结果。