Division of Metabolic Diseases, University of Groningen, University Medical Center Groningen, Beatrix Children's Hospital, Hanzeplein 1, 9713 GZ, Groningen, The Netherlands.
Department of Laboratory Medicine, Laboratory of Metabolic Diseases, University of Groningen, University Medical Center Groningen, Hanzeplein 1, 9713 GZ, Groningen, P.O. Box 30.001, 9700 RB, The Netherlands.
Orphanet J Rare Dis. 2020 Apr 3;15(1):82. doi: 10.1186/s13023-020-1343-7.
This study investigated the agreement between various dried blood spot (DBS) and venous blood sample measurements of phenylalanine and tyrosine concentrations in Phenylketonuria (PKU) and Tyrosinemia type 1 (TT1) patients.
Phenylalanine and tyrosine concentrations were studied in 45 PKU/TT1 patients in plasma from venous blood in lithium heparin (LH) and EDTA tubes; venous blood from LH and EDTA tubes on a DBS card; venous blood directly on a DBS card; and capillary blood on a DBS card. Plasma was analyzed with an amino acid analyzer and DBS were analyzed with liquid chromatography-mass spectrometry. Agreement between different methods was assessed using Passing and Bablok fit and Bland Altman analyses.
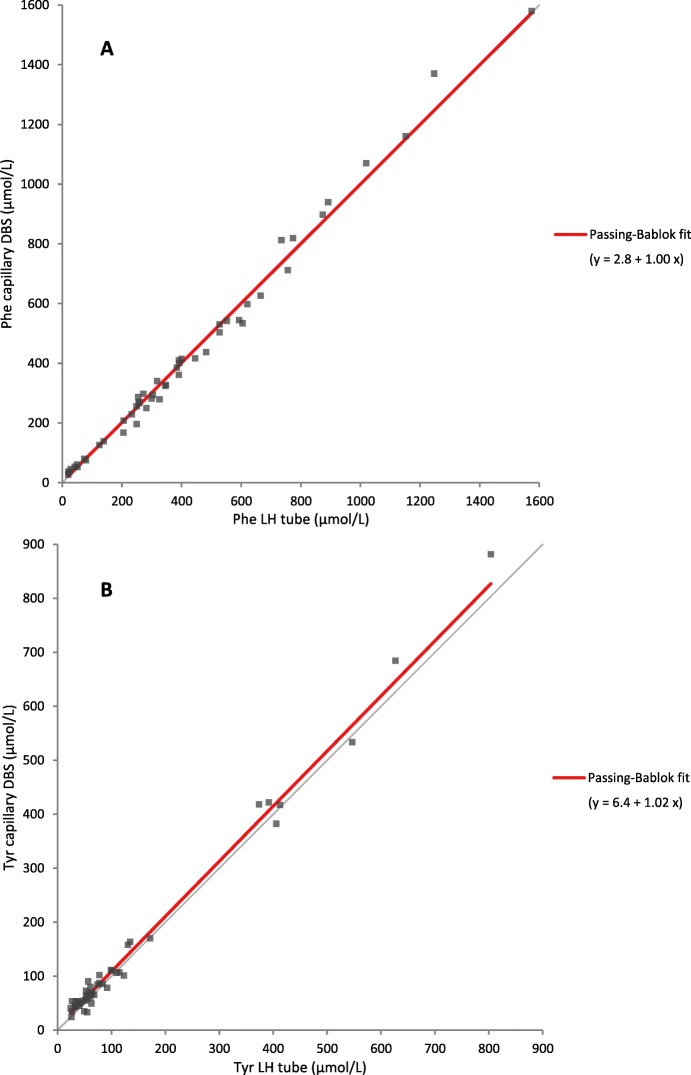
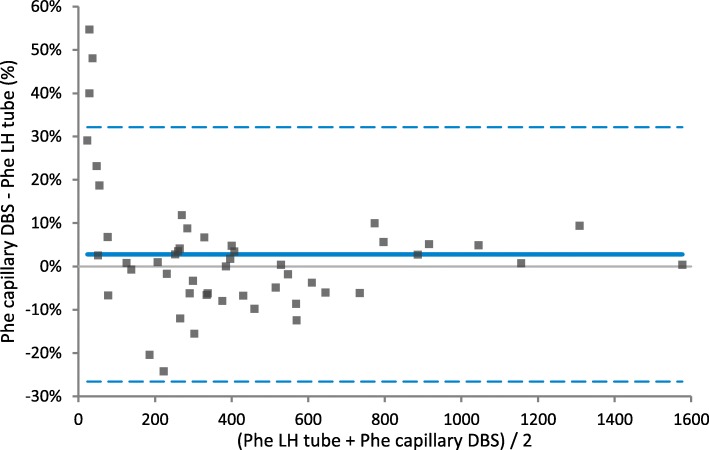
In general, phenylalanine concentrations in LH plasma were comparable to capillary DBS, whereas tyrosine concentrations were slightly higher in LH plasma (constant bias of 6.4 μmol/L). However, in the low phenylalanine range, most samples had higher phenylalanine concentrations in DBS compared to LH plasma. Remarkably, phenylalanine and tyrosine in EDTA plasma were higher compared to all other samples (slopes ranging from 7 to 12%). No differences were observed when comparing capillary DBS to other DBS.
Overall agreement between plasma and DBS is good. However, bias is specimen- (LH vs EDTA), and possibly concentration- (low phenylalanine) dependent. Because of the overall good agreement, we recommend the use of a DBS-plasma correction factor for DBS measurement. Each laboratory should determine their own factor dependent on filter card type, extraction and calibration protocols taking the LH plasma values as gold standard.
本研究调查了不同干血斑(DBS)与苯丙酮尿症(PKU)和酪氨酸血症 1 型(TT1)患者静脉血样中苯丙氨酸和酪氨酸浓度的 DBS 测量值之间的一致性。
对 45 例 PKU/TI1 患者的苯丙氨酸和酪氨酸浓度进行了研究,包括肝素锂(LH)和 EDTA 管中的静脉血血浆;DBS 卡上的 LH 和 EDTA 管中的静脉血;DBS 卡上的直接静脉血;DBS 卡上的毛细血管血。用氨基酸分析仪分析血浆,用液相色谱-质谱法分析 DBS。使用 Passing 和 Bablok 拟合以及 Bland Altman 分析评估不同方法之间的一致性。
一般来说,LH 血浆中的苯丙氨酸浓度与毛细血管 DBS 相当,而 LH 血浆中的酪氨酸浓度略高(恒偏 6.4μmol/L)。然而,在低苯丙氨酸范围内,与 LH 血浆相比,大多数样本中的 DBS 苯丙氨酸浓度更高。值得注意的是,EDTA 血浆中的苯丙氨酸和酪氨酸浓度与所有其他样本相比都更高(斜率范围为 7 至 12%)。比较毛细血管 DBS 与其他 DBS 时,未观察到差异。
总体而言,血浆与 DBS 之间的一致性良好。然而,偏倚与标本(LH 与 EDTA)有关,可能与浓度(低苯丙氨酸)有关。由于总体一致性良好,我们建议使用 DBS-血浆校正因子对 DBS 测量值进行校正。每个实验室都应根据滤光片卡类型、提取和校准方案确定自己的因子,以 LH 血浆值为金标准。