Badran Bashar W, Jenkins Dorothea D, Cook Daniel, Thompson Sean, Dancy Morgan, DeVries William H, Mappin Georgia, Summers Philipp, Bikson Marom, George Mark S
Department of Psychiatry, Medical University of South Carolina, Charleston, SC, United States.
Department of Pediatrics, Medical University of South Carolina, Charleston, SC, United States.
Front Hum Neurosci. 2020 Mar 18;14:77. doi: 10.3389/fnhum.2020.00077. eCollection 2020.
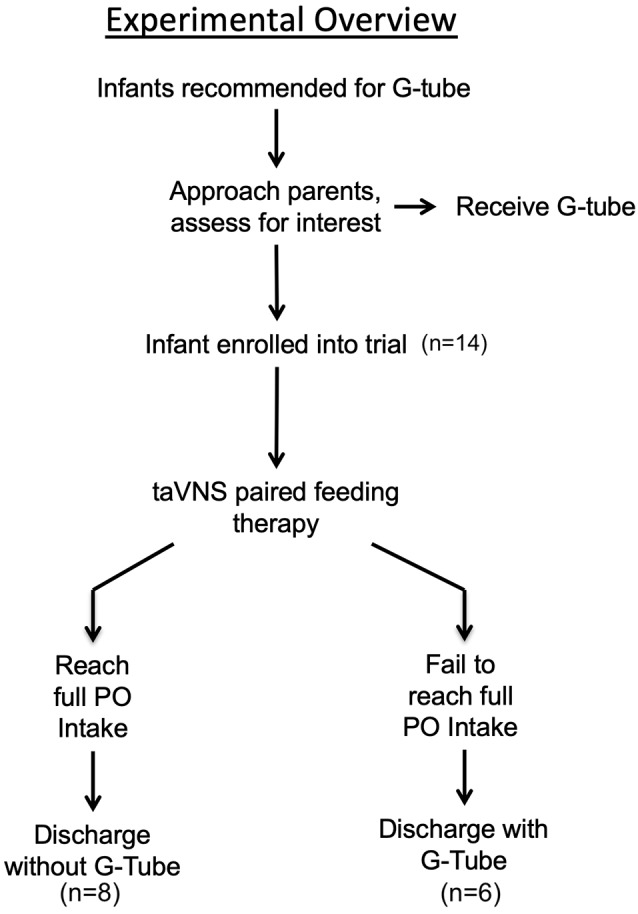
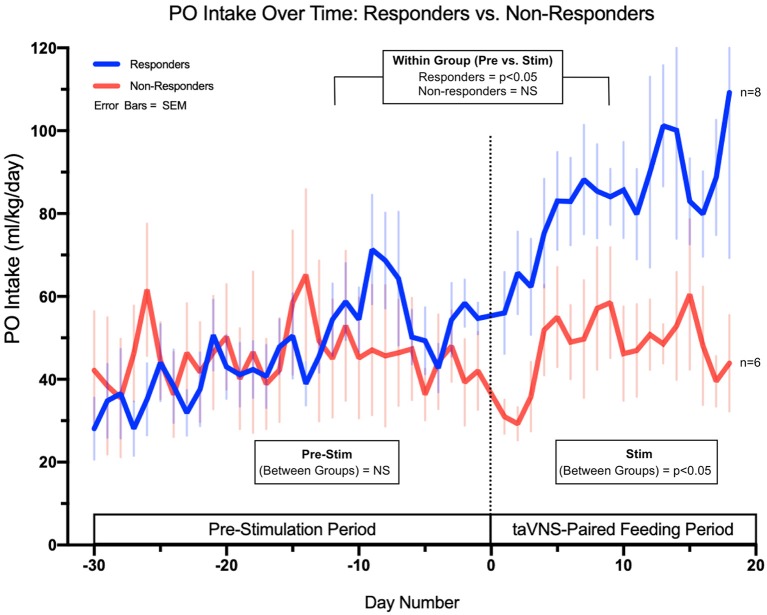
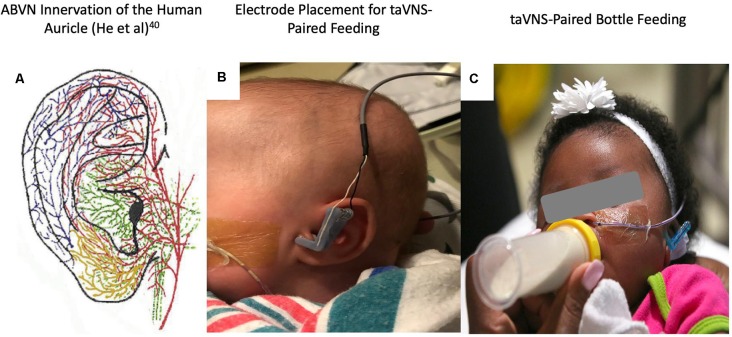
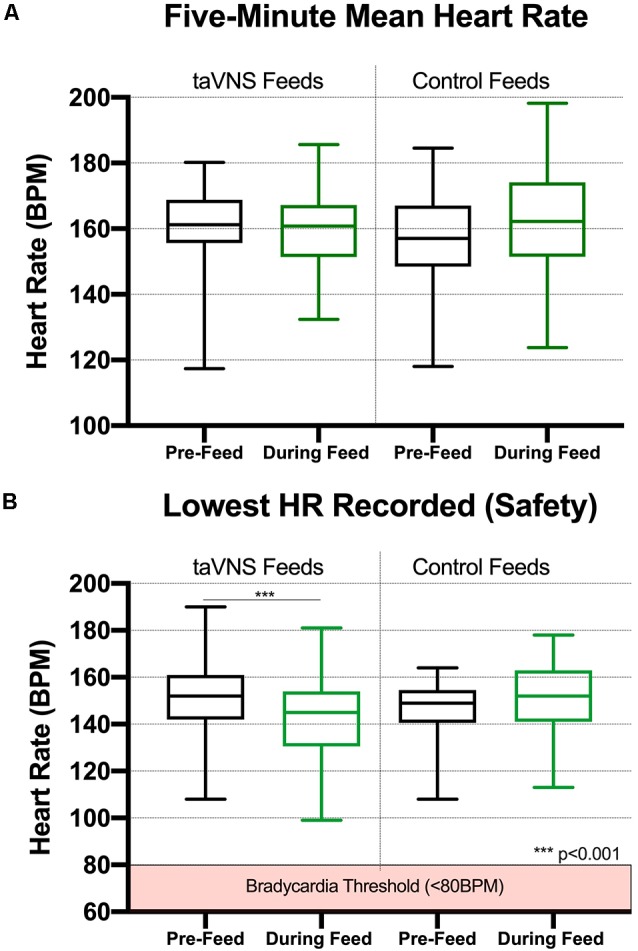
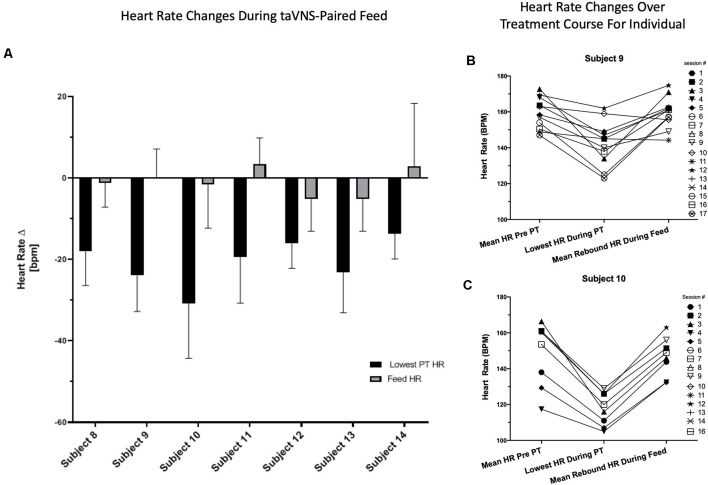
Neonates born premature or who suffer brain injury at birth often have oral feeding dysfunction and do not meet oral intake requirements needed for discharge. Low oral intake volumes result in extended stays in the hospital (>2 months) and can lead to surgical implant and explant of a gastrostomy tube (G-tube). Prior work suggests pairing vagus nerve stimulation (VNS) with motor activity accelerates functional improvements after stroke, and transcutaneous auricular VNS (taVNS) has emerged as promising noninvasive form of VNS. Pairing taVNS with bottle-feeding rehabilitation may improve oromotor coordination and lead to improved oral intake volumes, ultimately avoiding the need for G-tube placement. We investigated whether taVNS paired with oromotor rehabilitation is tolerable and safe and facilitates motor learning in infants who have failed oral feeding. We enrolled 14 infants [11 premature and 3 hypoxic-ischemic encephalopathy (HIE)] who were slated for G-tube placement in a prospective, open-label study of taVNS-paired rehabilitation to increase feeding volumes. Once-daily taVNS was delivered to the left tragus during bottle feeding for 2 weeks, with optional extension. The primary outcome was attainment of oral feeding volumes and weight gain adequate for discharge without G-tube while also monitoring discomfort and heart rate (HR) as safety outcomes. We observed no adverse events related to stimulation, and stimulation-induced HR reductions were transient and safe and likely confirmed vagal engagement. Eight of 14 participants (57%) achieved adequate feeding volumes for discharge without G-tube (mean treatment length: 16 ± 6 days). We observed significant increases in feeding volume trajectories in responders compared with pre-stimulation ( < 0.05). taVNS-paired feeding rehabilitation appears safe and may improve oral feeding in infants with oromotor dyscoordination, increasing the rate of discharge without G-tube, warranting larger controlled trials.
早产或出生时脑部受伤的新生儿通常存在经口喂养功能障碍,无法达到出院所需的经口摄入量要求。经口摄入量低会导致住院时间延长(超过2个月),并可能导致胃造口管(G管)的手术植入和拔除。先前的研究表明,将迷走神经刺激(VNS)与运动活动相结合可加速中风后的功能改善,而经皮耳迷走神经刺激(taVNS)已成为一种有前景的非侵入性VNS形式。将taVNS与奶瓶喂养康复相结合可能会改善口面部运动协调性,并导致经口摄入量增加,最终避免放置G管的需要。我们研究了taVNS与口面部运动康复相结合在经口喂养失败的婴儿中是否可耐受且安全,并是否有助于运动学习。我们招募了14名婴儿[11名早产儿和3名缺氧缺血性脑病(HIE)患儿],他们计划在一项关于taVNS配对康复以增加喂养量的前瞻性、开放标签研究中接受G管放置。在奶瓶喂养期间,每天一次将taVNS施加于左耳屏,持续2周,可选择延长。主要结局是达到足以出院且无需G管的经口喂养量和体重增加,同时监测不适和心率(HR)作为安全性结局。我们未观察到与刺激相关的不良事件,刺激引起的HR降低是短暂且安全的,可能证实了迷走神经的参与。14名参与者中有8名(57%)达到了足以出院且无需G管的喂养量(平均治疗时长:16±6天)。与刺激前相比,我们观察到反应者的喂养量轨迹有显著增加(<0.05)。taVNS配对喂养康复似乎是安全的,可能会改善口面部运动不协调婴儿的经口喂养,提高无需G管出院的比例,值得进行更大规模的对照试验。