Department of Surgery and Emory Critical Care Center, Emory University, Atlanta, GA, USA.
Chirec Hospitals, Université Libre de Bruxelles, Brussels, Belgium.
Intensive Care Med. 2018 Sep;44(9):1400-1426. doi: 10.1007/s00134-018-5175-z. Epub 2018 Jul 3.
To identify research priorities in the management, epidemiology, outcome and underlying causes of sepsis and septic shock.
A consensus committee of 16 international experts representing the European Society of Intensive Care Medicine and Society of Critical Care Medicine was convened at the annual meetings of both societies. Subgroups had teleconference and electronic-based discussion. The entire committee iteratively developed the entire document and recommendations.
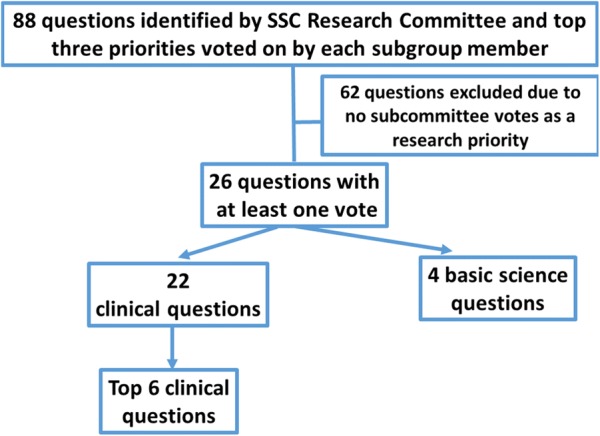
Each committee member independently gave their top five priorities for sepsis research. A total of 88 suggestions (ESM 1 - supplemental table 1) were grouped into categories by the committee co-chairs, leading to the formation of seven subgroups: infection, fluids and vasoactive agents, adjunctive therapy, administration/epidemiology, scoring/identification, post-intensive care unit, and basic/translational science. Each subgroup had teleconferences to go over each priority followed by formal voting within each subgroup. The entire committee also voted on top priorities across all subgroups except for basic/translational science.
The Surviving Sepsis Research Committee provides 26 priorities for sepsis and septic shock. Of these, the top six clinical priorities were identified and include the following questions: (1) can targeted/personalized/precision medicine approaches determine which therapies will work for which patients at which times?; (2) what are ideal endpoints for volume resuscitation and how should volume resuscitation be titrated?; (3) should rapid diagnostic tests be implemented in clinical practice?; (4) should empiric antibiotic combination therapy be used in sepsis or septic shock?; (5) what are the predictors of sepsis long-term morbidity and mortality?; and (6) what information identifies organ dysfunction?
While the Surviving Sepsis Campaign guidelines give multiple recommendations on the treatment of sepsis, significant knowledge gaps remain, both in bedside issues directly applicable to clinicians, as well as understanding the fundamental mechanisms underlying the development and progression of sepsis. The priorities identified represent a roadmap for research in sepsis and septic shock.
确定脓毒症和感染性休克管理、流行病学、结局和根本原因方面的研究重点。
代表欧洲危重病医学会和重症监护医学会的 16 位国际专家组成共识委员会,在两个学会的年会上召开会议。分组进行电话会议和电子讨论。整个委员会对整个文件和建议进行反复讨论。
每位委员会成员独立列出脓毒症研究的前五项重点。总共 88 条建议(ESM1-补充表 1)由委员会联合主席分组,形成七个分组:感染、液体和血管活性药物、辅助治疗、管理/流行病学、评分/识别、重症监护后和基础/转化科学。每个分组先进行电话会议讨论每个重点,然后在每个分组内进行正式投票。除基础/转化科学外,整个委员会还对所有分组的重点进行投票。
存活脓毒症研究委员会为脓毒症和感染性休克提供了 26 项重点。其中,确定了前 6 项临床重点,包括以下问题:(1)靶向/个性化/精准医学方法能否确定哪些治疗方法对哪些患者在哪些时间有效?;(2)容量复苏的理想终点是什么,应如何滴定容量复苏?;(3)快速诊断试验是否应在临床实践中实施?;(4)脓毒症或感染性休克是否应使用经验性抗生素联合治疗?;(5)脓毒症长期发病率和死亡率的预测因素有哪些?;(6)哪些信息可识别器官功能障碍?
尽管存活脓毒症运动指南对脓毒症的治疗提出了多项建议,但仍存在重大知识空白,包括直接适用于临床医生的床边问题,以及对脓毒症发展和进展的基本机制的理解。确定的重点代表了脓毒症和感染性休克研究的路线图。