Candemir Mustafa, Şahinarslan Asife, Yazol Merve, Öner Yusuf Ali, Boyacı Bülent
Yozgat City Hospital - Department of Cardiology , Yozgat - Turquia.
Gazi University - Faculty of Medicine - Department of Cardiology , Ankara - Turquia.
Arq Bras Cardiol. 2020 Mar;114(3):540-551. doi: 10.36660/abc.2018149.
Pathophysiology and prognosis are not clearly determined in patients with the coronary slow flow phenomenon (CSFP). These patients present with various clinical conditions ranging from being asymptomatic to being admitted with sudden cardiac death.
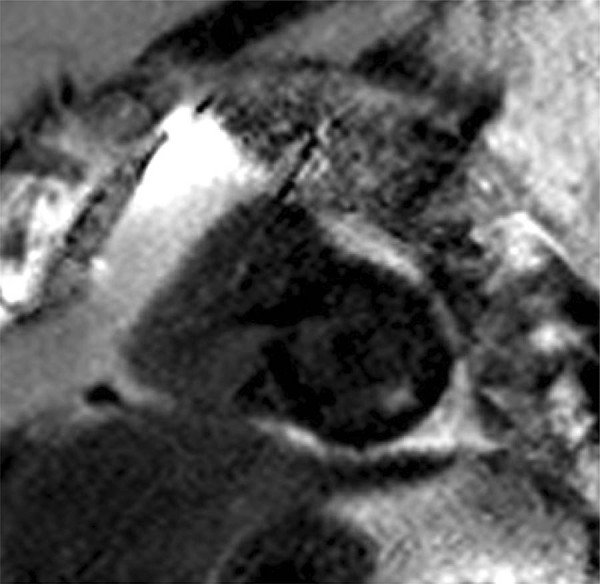
We aimed at assessing the findings of late gadolinium enhancement (LGE) in cardiac magnetic resonance imaging (CMR) as an indicator of myocardial fibrosis. We also aimed at determining the relationship between the presence of myocardial fibrosis and NT-proBNP levels in patients with CSFP in the left anterior descending coronary artery (LAD).
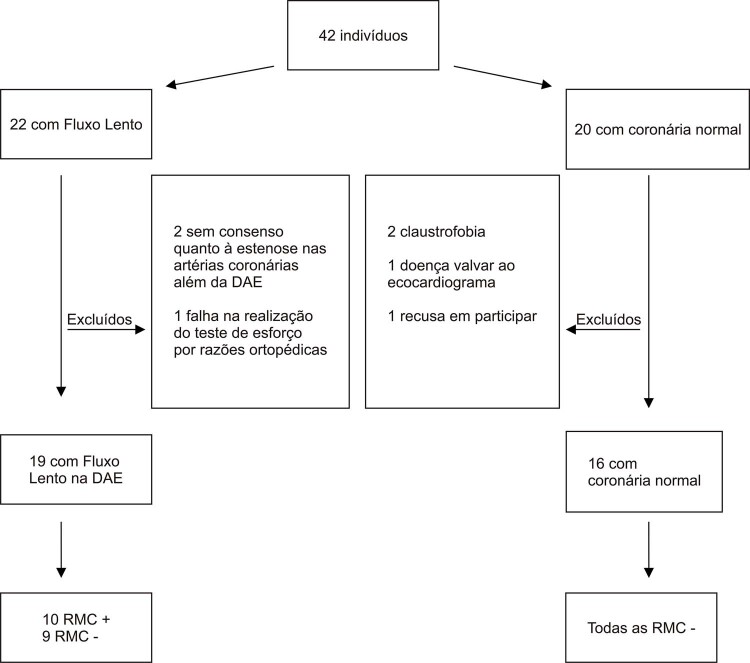
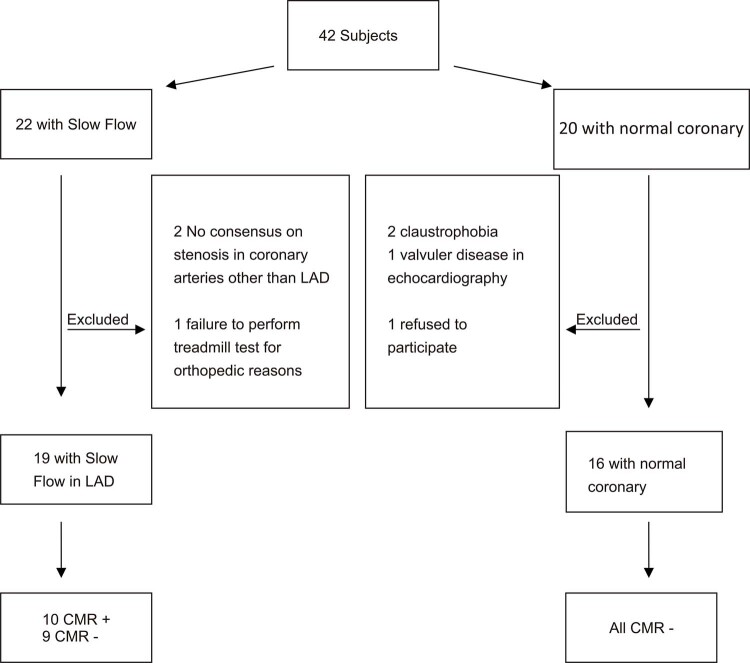
A total of 35 patients were enrolled within an age range of 31-75. The study patients (n=19) had normal epicardial coronary arteries at angiography, but they presented with CSFP in the LAD. The control group patients (n=16) had normal epicardial coronary arteries and TIMI scores at normal levels in angiography. In both groups, the patients were examined with CMR for the presence of myocardial fibrosis. In addition, plasma NT-proBNP levels were measured. A p-value < 0.05 was considered significant.
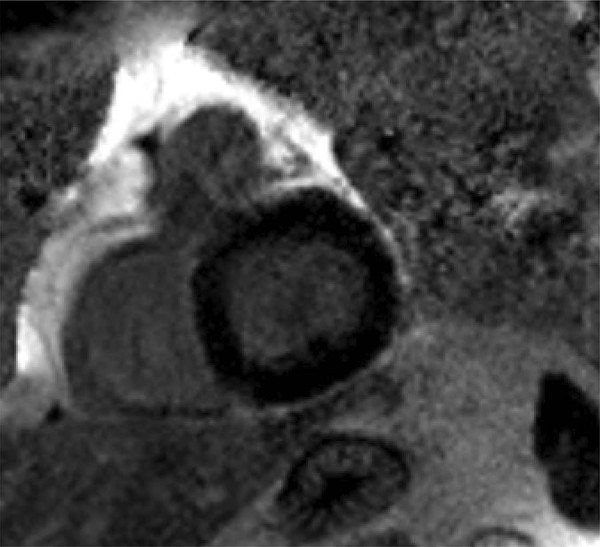
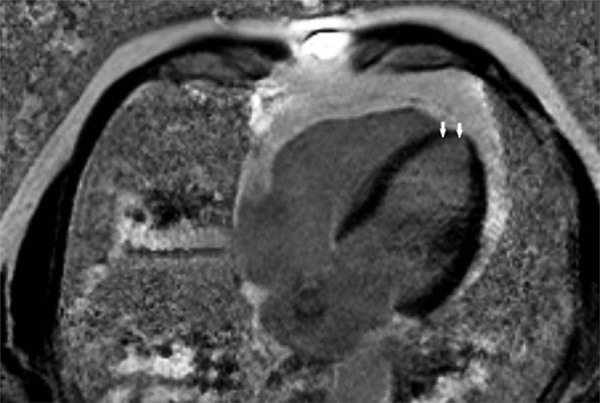
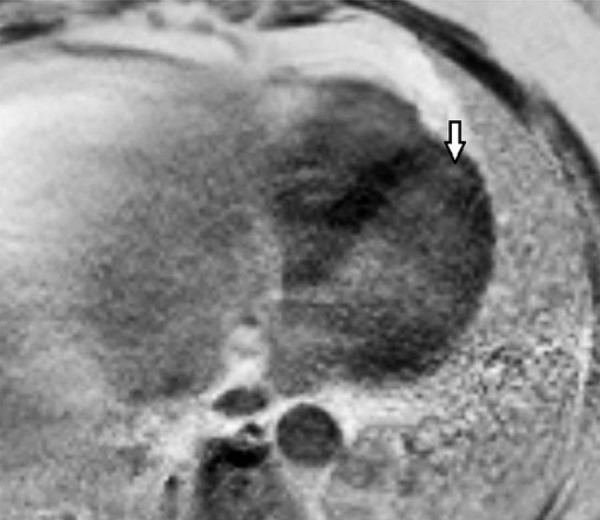
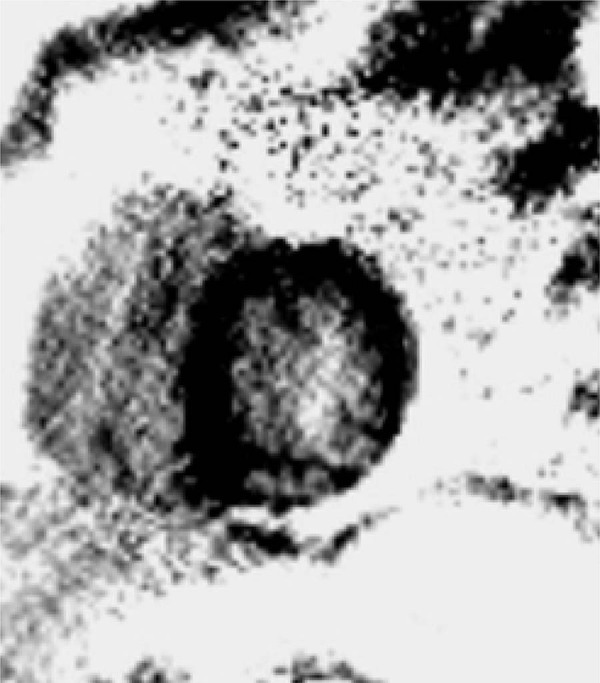
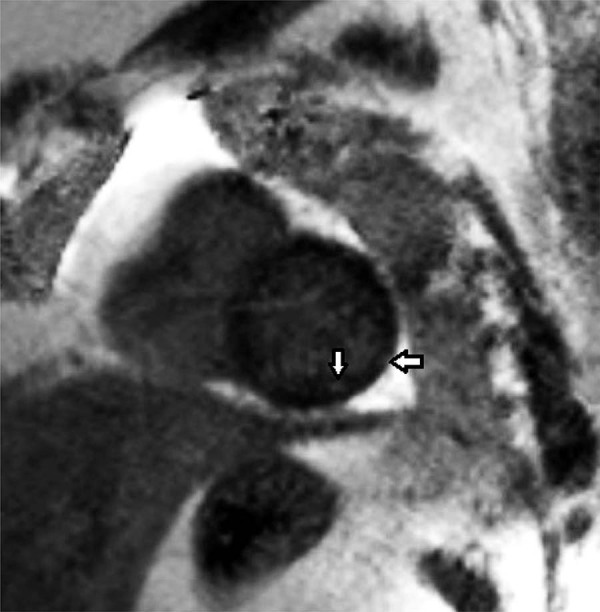
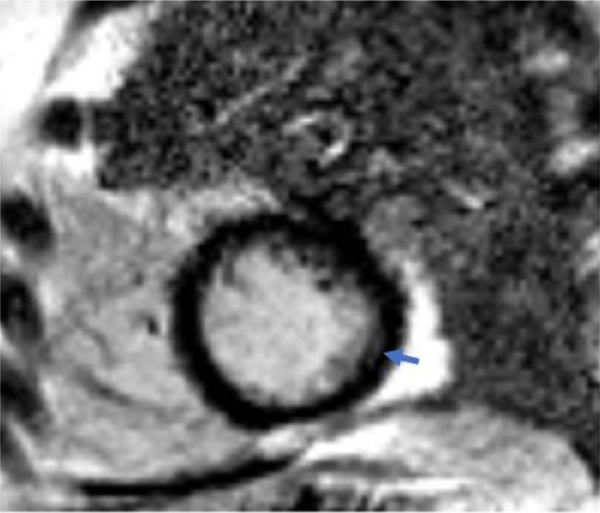
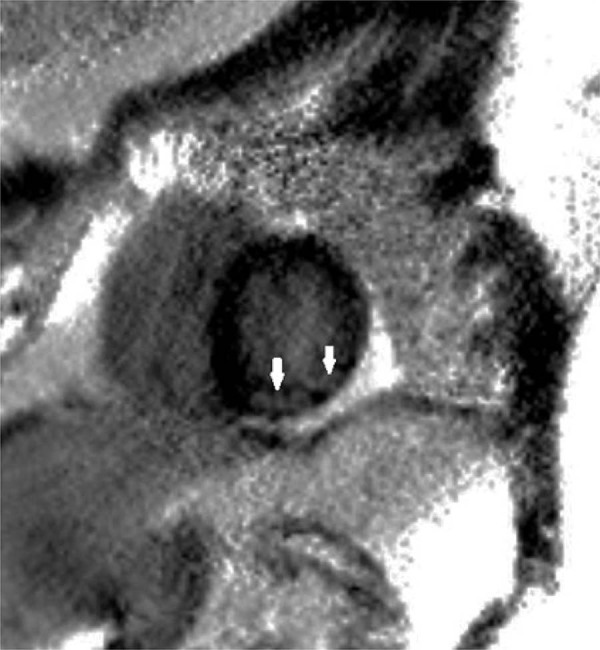
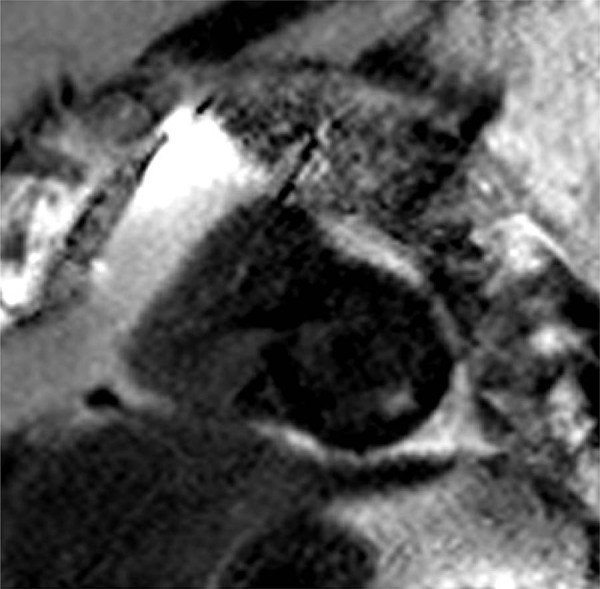
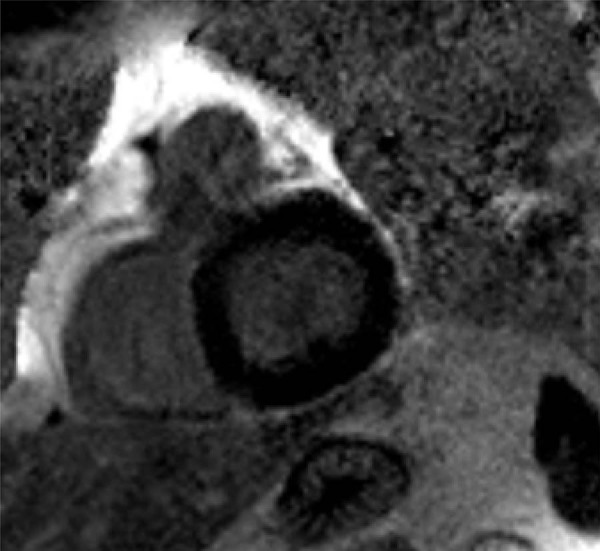
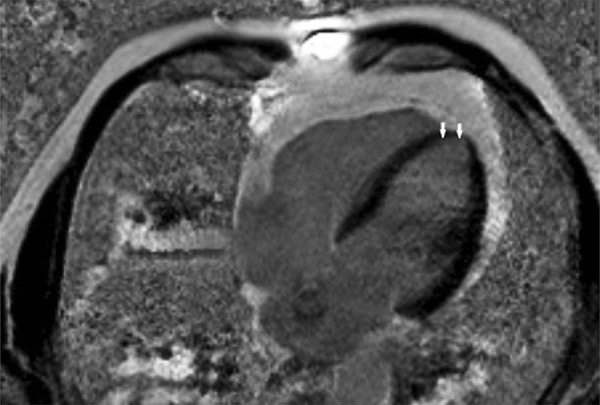
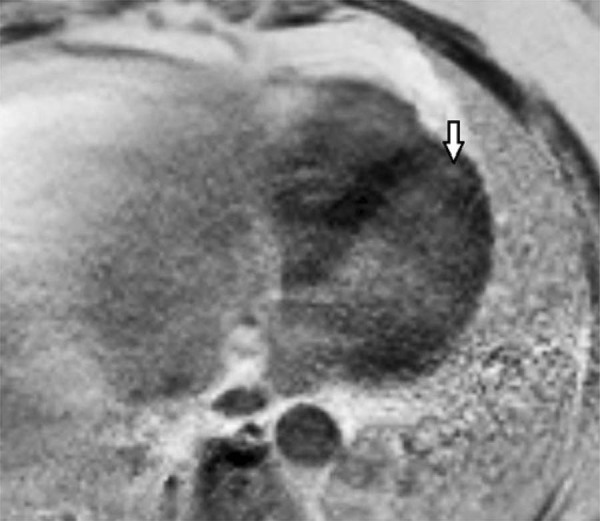
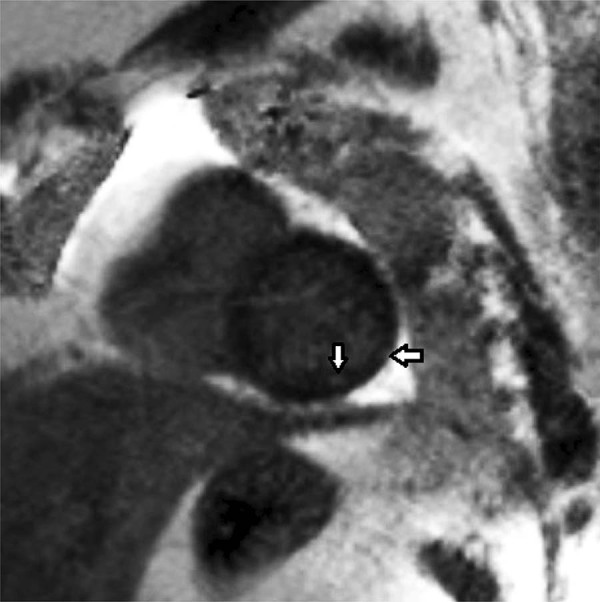
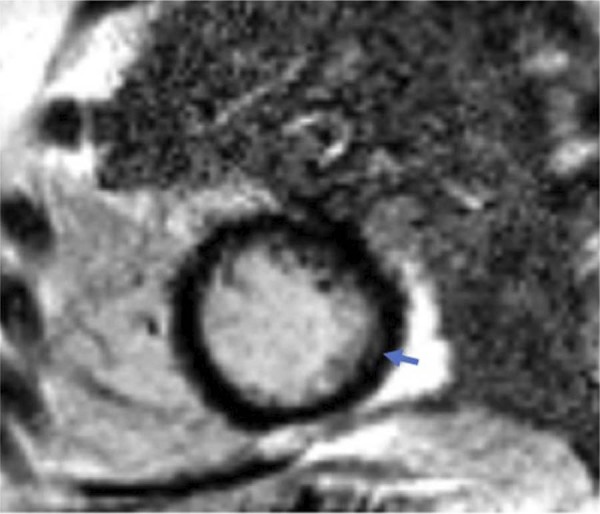
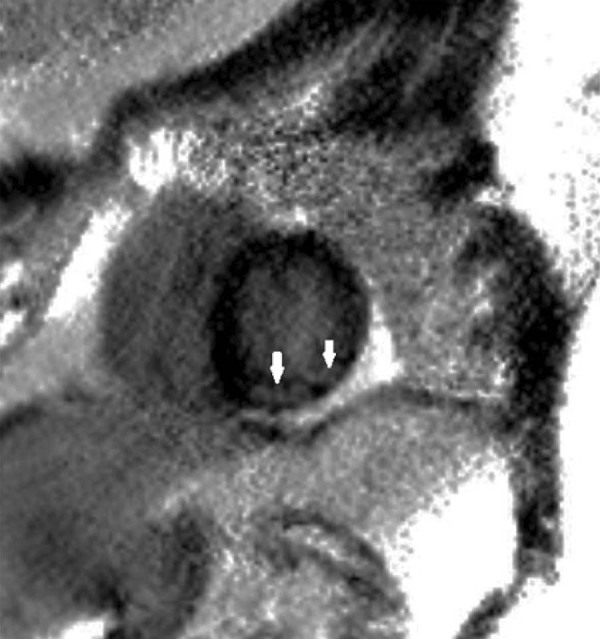
The rate of myocardial fibrosis was significantly higher in CMR in the patients with CSFP (p=0.018). A variable amount of myocardial scar tissue was detected at the left ventricular apex in 7 patients and at the inferior and inferolateral regions in 3 patients. There was no difference in the level of NT-proBNP in patients with CSFP. However, the NT-proBNP levels were higher in patients with CSFP, who had scar tissue in CMR (p=0.022).
In conclusion, LGE in CMR showed that ischemic myocardial scarring may exist in patients with CSFP. These results indicate that CSFP may not always be innocent. (Arq Bras Cardiol. 2020; 114(3):540-551).
冠状动脉慢血流现象(CSFP)患者的病理生理学和预后尚未明确确定。这些患者表现出各种临床情况,从无症状到因心源性猝死入院。
我们旨在评估心脏磁共振成像(CMR)中的延迟钆增强(LGE)结果作为心肌纤维化的指标。我们还旨在确定左前降支冠状动脉(LAD)中CSFP患者的心肌纤维化与NT-proBNP水平之间的关系。
共纳入35例年龄在31至75岁之间的患者。研究患者(n = 19)在血管造影时心外膜冠状动脉正常,但在LAD中表现出CSFP。对照组患者(n = 16)心外膜冠状动脉正常,血管造影时TIMI评分正常。两组患者均接受CMR检查以确定是否存在心肌纤维化。此外,测量血浆NT-proBNP水平。p值<0.05被认为具有统计学意义。
CSFP患者CMR中心肌纤维化的发生率显著更高(p = 0.018)。在7例患者的左心室心尖和3例患者的下壁及下侧壁区域检测到不同程度的心肌瘢痕组织。CSFP患者的NT-proBNP水平无差异。然而,CMR中有瘢痕组织的CSFP患者的NT-proBNP水平更高(p = 0.022)。
总之,CMR中的LGE显示CSFP患者可能存在缺血性心肌瘢痕。这些结果表明CSFP可能并不总是无害的。(《巴西心脏病学杂志》。2020;114(3):540 - 551)