Schlicker Sandra, Baumeister Harald, Buntrock Claudia, Sander Lasse, Paganini Sarah, Lin Jiaxi, Berking Matthias, Lehr Dirk, Ebert David Daniel
Department of Clinical Psychology and Psychotherapy, Friedrich-Alexander-University Erlangen-Nürnberg, Erlangen, Germany.
Department of Clinical Psychology and Psychotherapy, Philipps-University Marburg, Marburg, Germany.
JMIR Ment Health. 2020 Apr 15;7(4):e16398. doi: 10.2196/16398.
Chronic back pain (CBP) is linked to a higher prevalence and higher occurrence of major depressive disorder (MDD) and can lead to reduced quality of life. Unfortunately, individuals with both CBP and recurrent MDD are underidentified. Utilizing health care insurance data may provide a possibility to better identify this complex population. In addition, internet- and mobile-based interventions might enhance the availability of existing treatments and provide help to those highly burdened individuals.
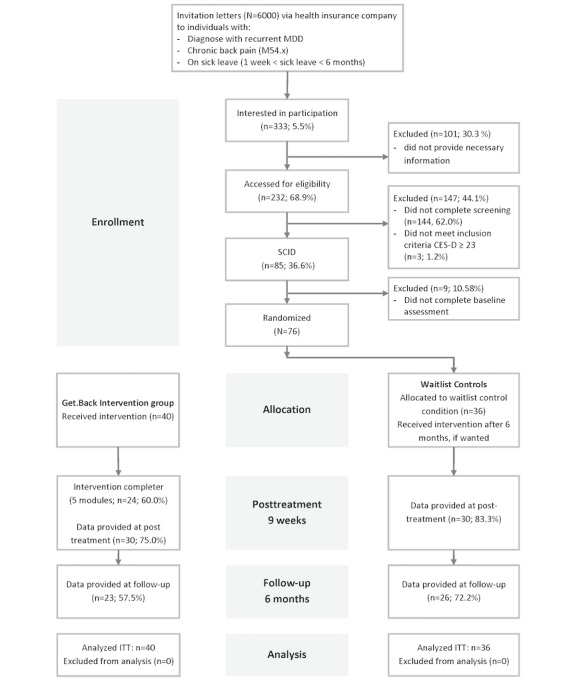
This pilot randomized controlled trial investigated the feasibility of recruitment via the health records of a German health insurance company. The study also examined user satisfaction and effectiveness of a 9-week cognitive behavioral therapy and Web- and mobile-based guided self-help intervention Get.Back in CBP patients with recurrent MDD on sick leave compared with a waitlist control condition.
Health records from a German health insurance company were used to identify and recruit participants (N=76) via invitation letters. Study outcomes were measured using Web-based self-report assessments at baseline, posttreatment (9 weeks), and a 6-month follow-up. The primary outcome was depressive symptom severity (Center for Epidemiological Studies-Depression); secondary outcomes included anxiety (Hamilton Anxiety and Depression Scale), quality of life (Assessment of Quality of Life), pain-related variables (Oswestry Disability Index, Pain Self-Efficacy Questionnaire, and pain intensity), and negative effects (Inventory for the Assessment of Negative Effects of Psychotherapy).
The total enrollment rate with the recruitment strategy used was 1.26% (76/6000). Participants completed 4.8 modules (SD 2.6, range 0-7) of Get.Back. The overall user satisfaction was favorable (mean Client Satisfaction Questionnaire score=24.5, SD 5.2). Covariance analyses showed a small but statistically significant reduction in depressive symptom severity in the intervention group (n=40) at posttreatment compared with the waitlist control group (n=36; F=3.62, P=.03; d=0.28, 95% CI -0.17 to 0.74). Similar findings were noted for the reduction of anxiety symptoms (F=10.45; P=.001; d=0.14, 95% CI -0.31 to 0.60) at posttreatment. Other secondary outcomes were nonsignificant (.06≤P≤.44). At the 6-month follow-up, the difference between the groups with regard to reduction in depressive symptom severity was no longer statistically significant (F=1.50, P=.11; d=0.10, 95% CI -0.34 to 0.46). The between-group difference in anxiety at posttreatment was maintained to follow-up (F=2.94, P=.04; d=0.38, 95% CI -0.07 to 0.83). There were no statistically significant differences across groups regarding other secondary outcomes at the 6-month follow-up (.08≤P≤.42).
These results suggest that participants with comorbid depression and CBP on sick leave may benefit from internet- and mobile-based interventions, as exemplified with the positive user satisfaction ratings. The recruitment strategy via health insurance letter invitations appeared feasible, but more research is needed to understand how response rates in untreated individuals with CBP and comorbid depression can be increased.
German Clinical Trials Register DRKS00010820; https://www.drks.de/drks_web/navigate.do? navigationId=trial.HTML&TRIAL_ID=DRKS00010820.
慢性背痛(CBP)与重度抑郁症(MDD)的较高患病率和较高发生率相关,并且会导致生活质量下降。不幸的是,同时患有CBP和复发性MDD的个体未得到充分识别。利用医疗保险数据可能为更好地识别这一复杂人群提供一种可能性。此外,基于互联网和移动设备的干预措施可能会提高现有治疗方法的可及性,并为那些负担沉重的个体提供帮助。
这项试点随机对照试验调查了通过德国一家健康保险公司的健康记录进行招募的可行性。该研究还考察了与等待名单对照组相比,9周认知行为疗法以及基于网络和移动设备的自助引导干预措施“Get.Back”对休病假的复发性MDD的CBP患者的用户满意度和有效性。
使用德国一家健康保险公司的健康记录,通过邀请函识别并招募参与者(N = 76)。在基线、治疗后(9周)和6个月随访时,使用基于网络的自我报告评估来测量研究结果。主要结局是抑郁症状严重程度(流行病学研究中心抑郁量表);次要结局包括焦虑(汉密尔顿焦虑抑郁量表)、生活质量(生活质量评估)、疼痛相关变量(奥斯威斯残疾指数、疼痛自我效能问卷和疼痛强度)以及负面影响(心理治疗负面影响评估量表)。
所采用的招募策略的总招募率为1.26%(76/6000)。参与者完成了“Get.Back”的4.8个模块(标准差2.6,范围0 - 7)。总体用户满意度良好(客户满意度问卷平均得分 = 24.5,标准差5.2)。协方差分析显示,与等待名单对照组(n = 36)相比,干预组(n = 40)在治疗后抑郁症状严重程度有小幅但具有统计学意义的降低(F = 3.62,P = 0.03;d = 0.28,95%置信区间 - 0.17至0.74)。治疗后焦虑症状减轻也有类似发现(F = 10.45;P = 0.001;d = 0.14,95%置信区间 - 0.31至0.60)。其他次要结局无统计学意义(0.06≤P≤0.44)。在6个月随访时,两组在抑郁症状严重程度降低方面的差异不再具有统计学意义(F = 1.50,P = 0.11;d = 0.10,95%置信区间 - 0.34至0.46)。治疗后两组之间的焦虑差异在随访时仍然存在(F = 2.94,P = 0.04;d = 0.38,95%置信区间 - 0.07至0.83)。在6个月随访时,其他次要结局在两组之间无统计学显著差异(0.08≤P≤0.42)。
这些结果表明,休病假的合并抑郁症和CBP的参与者可能从基于互联网和移动设备的干预措施中受益,如积极的用户满意度评分所示。通过健康保险信函邀请的招募策略似乎可行,但需要更多研究来了解如何提高未接受治疗的CBP合并抑郁症个体的响应率。
德国临床试验注册中心DRKS00010820;https://www.drks.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00010820