Dubin Arnaldo, Loudet Cecilia, Kanoore Edul Vanina S, Osatnik Javier, Ríos Fernando, Vásquez Daniela, Pozo Mario, Lattanzio Bernardo, Pálizas Fernando, Klein Francisco, Piezny Damián, Rubatto Birri Paolo N, Tuhay Graciela, García Analía, Santamaría Analía, Zakalik Graciela, González Cecilia, Estenssoro Elisa
Servicio de Terapia Intensiva, Sanatorio Otamendi, Azcuénaga 870, C1115 AAB, Buenos Aires, Argentina.
Hospital Interzonal de Agudos San Martin de La Plata, La Plata, Buenos Aires, Argentina.
Ann Intensive Care. 2020 Apr 15;10(1):40. doi: 10.1186/s13613-020-00659-7.
Resuscitation of septic patients regarding goals, monitoring aspects and therapy is highly variable. Our aim was to characterize cardiovascular and fluid management of sepsis in Argentina, a low and middle-income country (LMIC). Furthermore, we sought to test whether the utilization of dynamic tests of fluid responsiveness, as a guide for fluid therapy after initial resuscitation in patients with persistent or recurrent hypoperfusion, was associated with decreased mortality.
Secondary analysis of a national, multicenter prospective cohort study (n = 787) fulfilling Sepsis-3 definitions. Epidemiological characteristics, hemodynamic management data, type of fluids and vasopressors administered, physiological variables denoting hypoperfusion, use of tests of fluid responsiveness, and outcomes, were registered. Independent predictors of mortality were identified with logistic regression analysis.
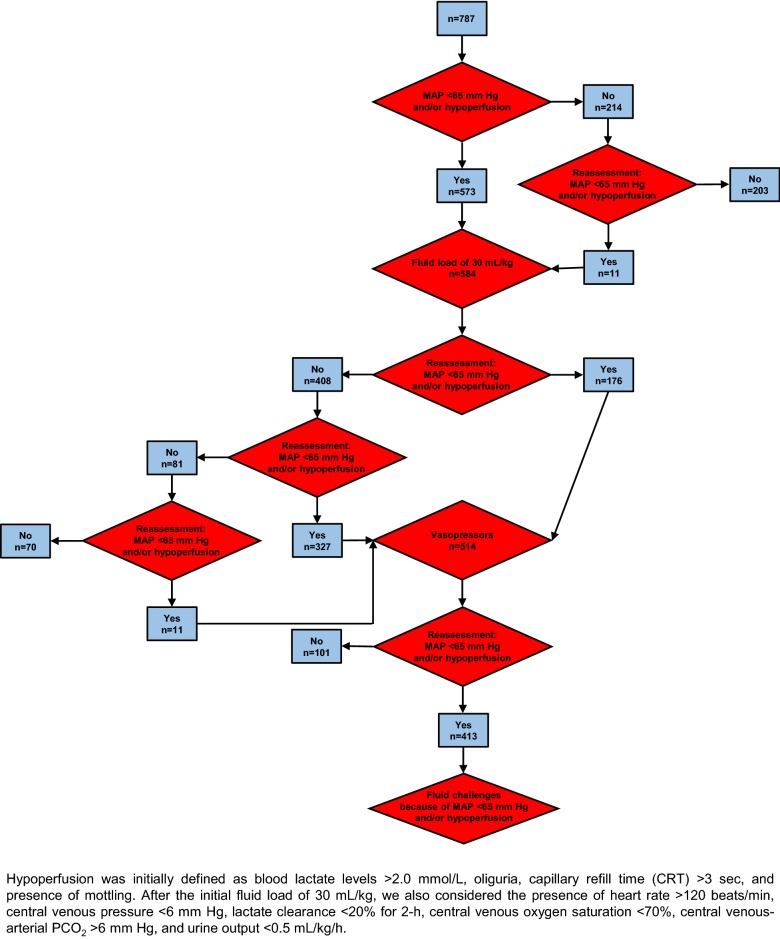
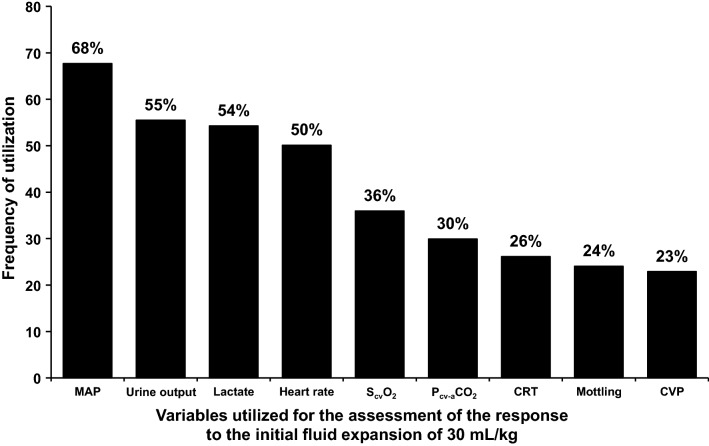
Initially, 584 of 787 patients (74%) had mean arterial pressure (MAP) < 65 mm Hg and/or signs of hypoperfusion and received 30 mL/kg of fluids, mostly normal saline (53%) and Ringer lactate (35%). Vasopressors and/or inotropes were administered in 514 (65%) patients, mainly norepinephrine (100%) and dobutamine (9%); in 22%, vasopressors were administered before ending the fluid load. After this, 413 patients (53%) presented persisting or recurrent hypotension and/or hypoperfusion, which prompted administration of additional fluid, based on: lactate levels (66%), urine output (62%), heart rate (54%), central venous O saturation (39%), central venous-arterial PCO difference (38%), MAP (31%), dynamic tests of fluid responsiveness (30%), capillary-refill time (28%), mottling (26%), central venous pressure (24%), cardiac index (13%) and/or pulmonary wedge pressure (3%). Independent predictors of mortality were SOFA and Charlson scores, lactate, requirement of mechanical ventilation, and utilization of dynamic tests of fluid responsiveness.
In this prospective observational study assessing the characteristics of resuscitation of septic patients in Argentina, a LMIC, the prevalent use of initial fluid bolus with normal saline and Ringer lactate and the use of norepinephrine as the most frequent vasopressor, reflect current worldwide practices. After initial resuscitation with 30 mL/kg of fluids and vasopressors, 413 patients developed persistent or recurrent hypoperfusion, which required further volume expansion. In this setting, the assessment of fluid responsiveness with dynamic tests to guide fluid resuscitation was independently associated with decreased mortality.
脓毒症患者在复苏目标、监测方面和治疗上存在很大差异。我们的目的是描述阿根廷这个低收入和中等收入国家(LMIC)脓毒症患者的心血管和液体管理情况。此外,我们试图检验在持续性或复发性低灌注患者初始复苏后,使用液体反应性动态测试作为液体治疗的指导是否与死亡率降低相关。
对一项符合脓毒症-3定义的全国性、多中心前瞻性队列研究(n = 787)进行二次分析。记录流行病学特征、血流动力学管理数据、给予的液体和血管加压药类型、表示低灌注的生理变量、液体反应性测试的使用情况以及结局。通过逻辑回归分析确定死亡率的独立预测因素。
最初,787例患者中有584例(74%)平均动脉压(MAP)< 65 mmHg和/或有低灌注体征,接受了30 mL/kg的液体,大部分为生理盐水(53%)和乳酸林格液(35%)。514例(65%)患者使用了血管加压药和/或正性肌力药,主要是去甲肾上腺素(100%)和多巴酚丁胺(9%);22%的患者在液体负荷结束前就使用了血管加压药。此后,413例患者(53%)出现持续性或复发性低血压和/或低灌注,这促使根据以下因素给予额外液体:乳酸水平(66%)、尿量(62%)、心率(54%)、中心静脉血氧饱和度(39%)、中心静脉-动脉二氧化碳分压差(38%)、MAP(31%)、液体反应性动态测试(30%)、毛细血管再充盈时间(28%)、皮肤花斑(26%)、中心静脉压(24%)、心脏指数(13%)和/或肺楔压(3%)。死亡率的独立预测因素是序贯器官衰竭评估(SOFA)和Charlson评分、乳酸、机械通气需求以及液体反应性动态测试的使用情况。
在这项评估阿根廷这个低收入和中等收入国家脓毒症患者复苏特征的前瞻性观察性研究中,普遍使用生理盐水和乳酸林格液进行初始液体推注以及最常使用去甲肾上腺素作为血管加压药,反映了当前的全球实践。在使用30 mL/kg液体和血管加压药进行初始复苏后,413例患者出现持续性或复发性低灌注,这需要进一步扩容。在这种情况下,使用动态测试评估液体反应性以指导液体复苏与死亡率降低独立相关。