University of Western Ontario, London, ON, Canada.
AbbVie, Inc, North Chicago, IL, USA.
Adv Ther. 2020 May;37(5):2356-2372. doi: 10.1007/s12325-020-01303-3. Epub 2020 Apr 15.
Janus kinase (JAK) inhibitors are a class of targeted therapies for rheumatoid arthritis (RA) with established clinical efficacy. However, little is known about their efficacy compared with each other. This network meta-analysis (NMA) estimated the comparative efficacy of JAK inhibitors currently approved for RA.
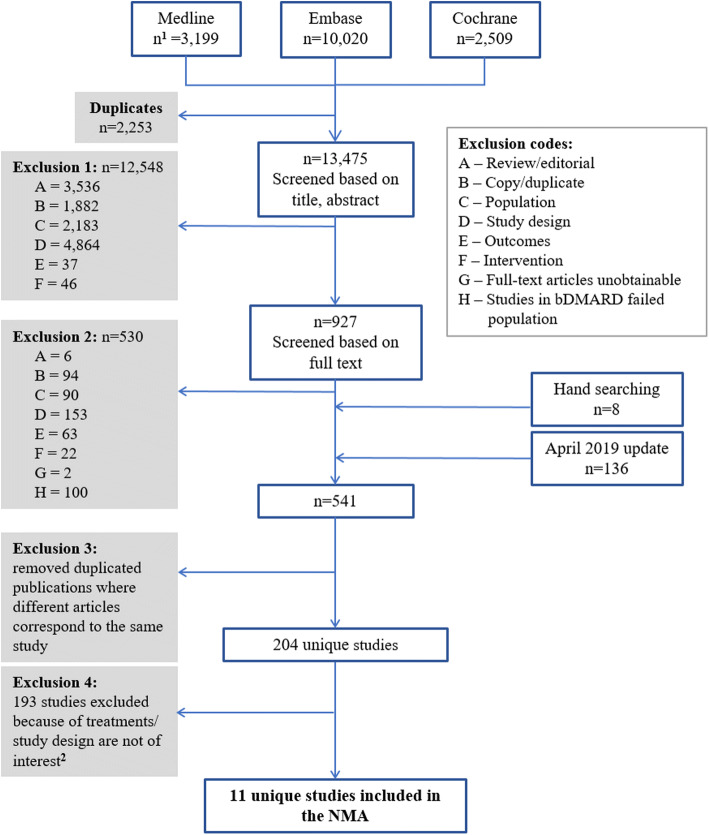
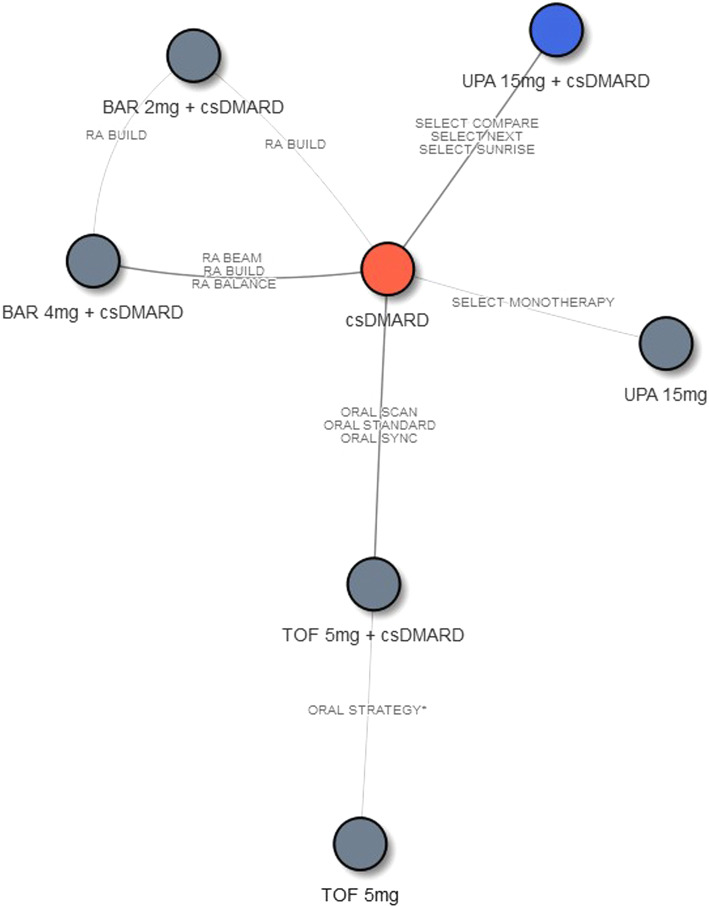
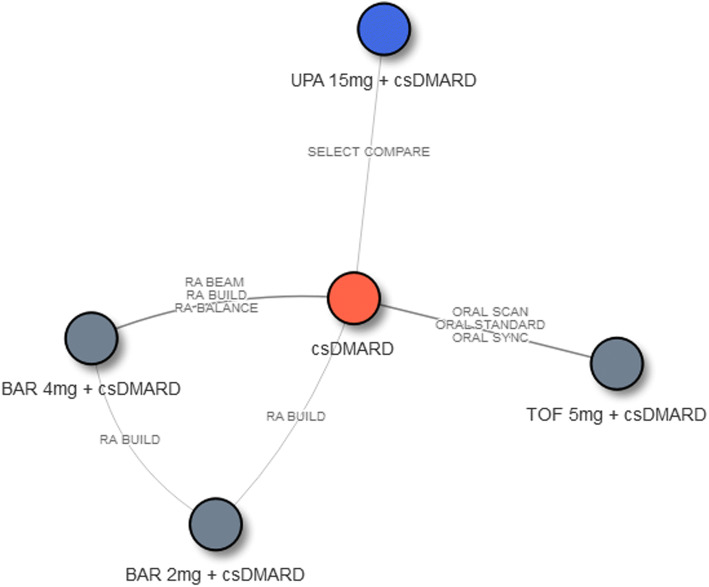
A targeted literature review was conducted for phase III randomized controlled trials (RCTs) evaluating the efficacy of three approved JAK inhibitors (tofacitinib, baricitinib, and upadacitinib) as monotherapy or combination therapy among patients with moderate-to-severe RA who had inadequate response to conventional synthetic disease-modifying antirheumatic drugs (csDMARD-IR). Using Bayesian NMA, American College of Rheumatology (ACR) 20/50/70 responses and clinical remission (defined as DAS28-CRP < 2.6) were evaluated separately at 12 and 24 weeks.
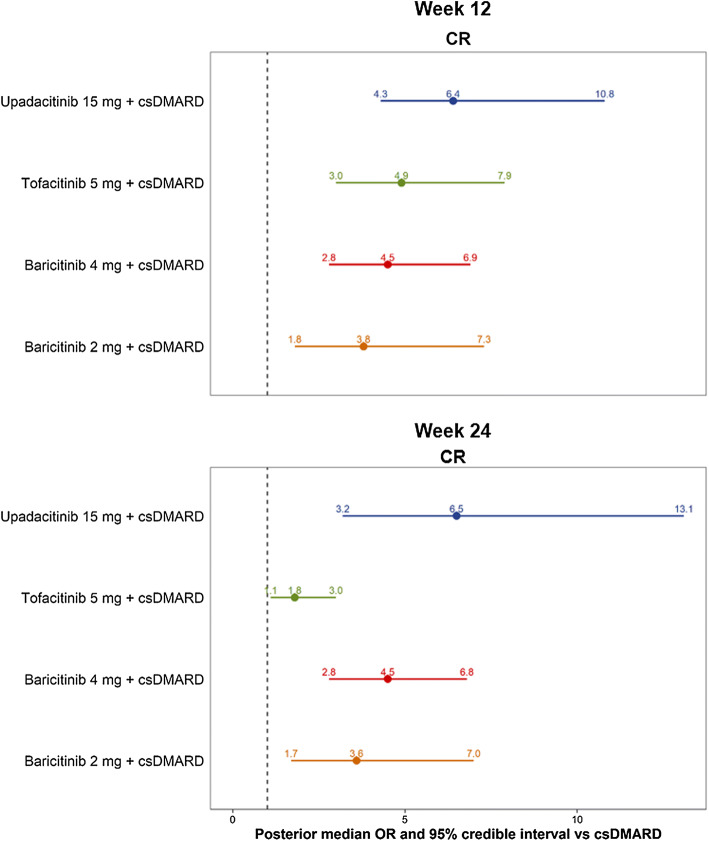
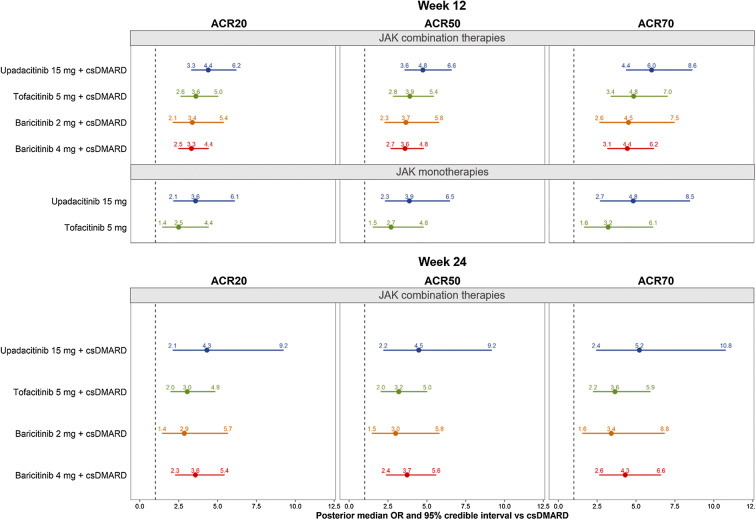
Eleven RCTs were identified and included in the NMA. All JAK inhibitors demonstrated significantly better efficacy than csDMARD. Among combination therapies, upadacitinib 15 mg had the highest 12-week ACR50 responses (median [95% credible interval]: 43.4% [33.4%, 54.5%]), followed by tofacitinib 5 mg (38.7% [28.6%, 49.8%]), baricitinib 2 mg (37.1% [25.0%, 50.6%]), and baricitinib 4 mg (36.7%, [27.2%, 47.0%]). Similar results were observed for ACR20/70 and at week 24. Upadacitinib 15 mg + csDMARD was also found to have the highest clinical remission rates at week 12 (29.8% [16.9%, 47.0%]), followed by tofacitinib 5 mg (24.3%, [12.7%, 40.2%]), baricitinib 4 mg (22.8%, [11.8%, 37.5%]), and baricitinib 2 mg (20.1%, [8.6%, 37.4%]). Similar results were seen at week 24. Among monotherapies, upadacitinib had a higher ACR50 response (38.5% [25.3%, 53.2%]) than tofacitinib (30.4% [18.3%, 45.5%]). The differences in efficacy measures were not statistically significant between the JAK inhibitors.
The NMA found that upadacitinib 15 mg once daily had numerically higher efficacy in terms of ACR response and clinical remission among approved JAK combination therapies and monotherapies for csDMARD-IR patients with RA.
Janus 激酶 (JAK) 抑制剂是一类针对类风湿关节炎 (RA) 的靶向治疗药物,具有明确的临床疗效。然而,目前对于这些药物之间的疗效比较知之甚少。本项网状荟萃分析(NMA)旨在评估目前已获批用于治疗对常规合成疾病修饰抗风湿药物 (csDMARD-IR) 反应不足的中重度 RA 患者的三种 JAK 抑制剂(托法替布、巴瑞替尼和乌帕替尼)的疗效。采用贝叶斯 NMA,分别在 12 周和 24 周评估美国风湿病学会 (ACR) 20/50/70 缓解和临床缓解(定义为 DAS28-CRP < 2.6)作为单药或联合治疗的疗效。
针对评估三种获批 JAK 抑制剂(托法替布、巴瑞替尼和乌帕替尼)作为单药或联合治疗对 csDMARD-IR 患者疗效的 III 期随机对照试验(RCT)进行了有针对性的文献回顾。这些 RCT 纳入了中重度 RA 患者,这些患者对 csDMARD 反应不足。采用贝叶斯 NMA,分别在 12 周和 24 周评估美国风湿病学会(ACR)20/50/70 缓解和临床缓解(定义为 DAS28-CRP < 2.6)作为单药或联合治疗的疗效。
共确定了 11 项 RCT 并纳入了 NMA。所有 JAK 抑制剂均显示出优于 csDMARD 的显著疗效。在联合治疗中,乌帕替尼 15mg 在 12 周时具有最高的 ACR50 缓解率(中位数 [95%可信区间]:43.4% [33.4%,54.5%]),其次是托法替布 5mg(38.7% [28.6%,49.8%])、巴瑞替尼 2mg(37.1% [25.0%,50.6%])和巴瑞替尼 4mg(36.7% [27.2%,47.0%])。在 ACR20/70 和 24 周时也观察到类似的结果。在 12 周时,乌帕替尼 15mg+csDMARD 还具有最高的临床缓解率(29.8% [16.9%,47.0%]),其次是托法替布 5mg(24.3% [12.7%,40.2%])、巴瑞替尼 4mg(22.8% [11.8%,37.5%])和巴瑞替尼 2mg(20.1% [8.6%,37.4%])。在 24 周时也观察到类似的结果。在单药治疗中,乌帕替尼的 ACR50 缓解率(38.5% [25.3%,53.2%])高于托法替布(30.4% [18.3%,45.5%])。这些 JAK 抑制剂之间的疗效差异无统计学意义。
本 NMA 发现,乌帕替尼 15mg 每日一次在获批用于治疗 csDMARD-IR 患者的 JAK 联合治疗和单药治疗中,在 ACR 缓解和临床缓解方面具有更高的疗效。