Selker Harry P, Welch Lisa C, Patchen-Fowler Elizabeth, Breeze Janis L, Terrin Norma, Parajulee Anshu, LeClair Amy, Naeim Arash, Marnocha Rebecca, Morelli Novak Julie, Caldwell Christine Sego, Cola Philip A, Croker Jennifer A, Cifu David X, Williams Kirsten M, Snyder Denise C, Kitterman Darlene
Tufts Clinical and Translational Science Institute, Tufts University, Boston, MA, USA.
Institute for Clinical Research and Health Policy Studies, Tufts Medical Center, Boston, MA, USA.
J Clin Transl Sci. 2020 Jan 27;4(2):115-124. doi: 10.1017/cts.2019.439. eCollection 2020 Apr.
Scientific quality and feasibility are part of ethics review by Institutional Review Boards (IRBs). Scientific Review Committees (SRCs) were proposed to facilitate this assessment by the Clinical and Translational Science Award (CTSA) SRC Consensus Group. This study assessed SRC feasibility and impact at CTSA-affiliated academic health centers (AHCs).
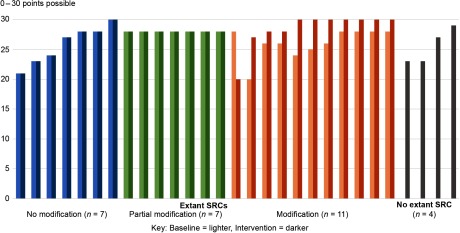
SRC implementation at 10 AHCs was assessed pre/post-intervention using quantitative and qualitative methods. Pre-intervention, four AHCs had no SRC, and six had at least one SRC needing modifications to better align with Consensus Group recommendations.
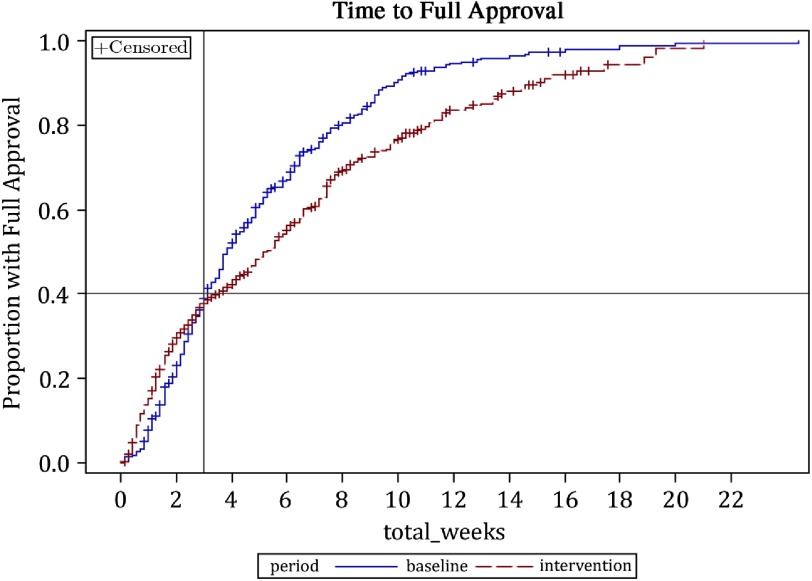
Facilitators of successful SRC implementation included broad-based communication, an external motivator, senior-level support, and committed SRC reviewers. Barriers included limited resources and staffing, variable local mandates, limited SRC authority, lack of anticipated benefit, and operational challenges. Research protocol quality did not differ significantly between study periods, but respondents suggested positive effects. During intervention, median total review duration did not lengthen for the 40% of protocols approved within 3 weeks. For the 60% under review after 3 weeks, review was lengthened primarily due to longer IRB review for SRC-reviewed protocols. Site interviews recommended designing locally effective SRC processes, building buy-in by communication or by mandate, allowing time for planning and sharing best practices, and connecting SRC and IRB procedures.
The CTSA SRC Consensus Group recommendations appear feasible. Although not conclusive in this relatively short initial implementation, sites perceived positive impact by SRCs on study quality. Optimal benefit will require local or federal mandate for implementation, adapting processes to local contexts, and employing SRC stipulations.
科学质量和可行性是机构审查委员会(IRB)伦理审查的一部分。临床与转化科学奖(CTSA)科学审查委员会(SRC)共识小组提议设立科学审查委员会以促进此项评估。本研究评估了CTSA附属学术健康中心(AHC)的SRC可行性及其影响。
采用定量和定性方法,在干预前后评估了10个AHC的SRC实施情况。干预前,4个AHC没有SRC,6个AHC至少有一个SRC需要修改,以更好地符合共识小组的建议。
SRC成功实施的促进因素包括广泛的沟通、外部激励因素、高层支持以及敬业的SRC评审员。障碍包括资源和人员有限、当地要求各异、SRC权力有限、缺乏预期效益以及运营挑战。研究方案质量在各研究阶段之间没有显著差异,但受访者表示有积极影响。在干预期间,3周内获批的40%的方案的总审查时长中位数没有延长。对于3周后仍在审查的60%的方案,审查时间延长主要是因为SRC审查的方案的IRB审查时间更长。现场访谈建议设计适合当地情况的SRC流程,通过沟通或强制要求获得支持,留出时间进行规划并分享最佳实践,以及将SRC和IRB程序联系起来。
CTSA SRC共识小组的建议似乎是可行的。尽管在这个相对较短的初步实施阶段尚无定论,但各机构认为SRC对研究质量有积极影响。要实现最佳效益,将需要地方或联邦强制实施,使流程适应当地情况,并采用SRC规定。