Division of Critical Care Medicine Department of Anesthesiology and Critical Care Medicine Children's Hospital of Philadelphia PA.
Division of Neurology Department of Pediatrics Children's Hospital of Philadelphia PA.
J Am Heart Assoc. 2020 May 5;9(9):e015032. doi: 10.1161/JAHA.119.015032. Epub 2020 Apr 23.
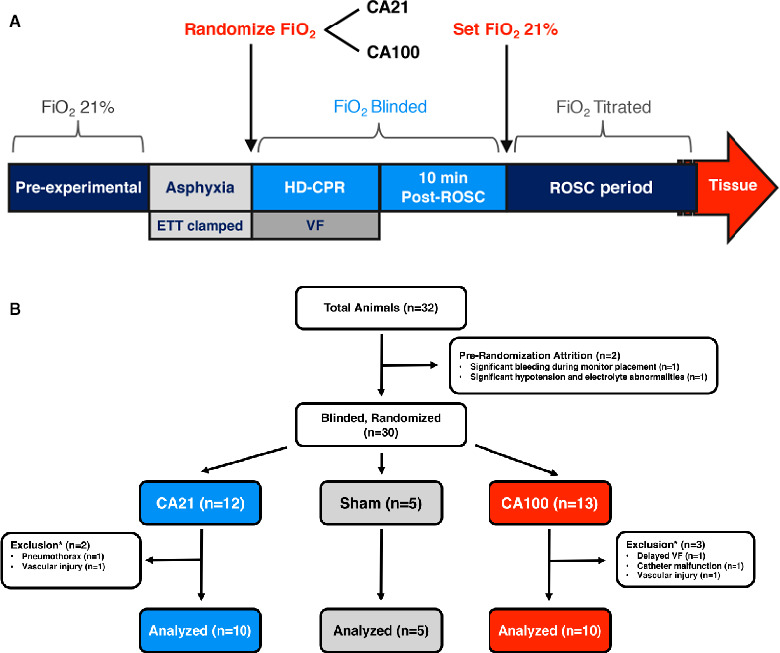
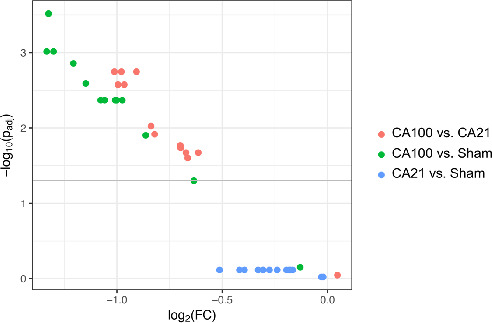
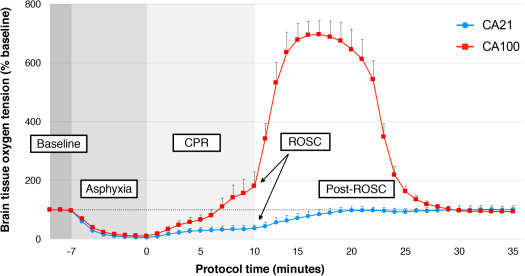
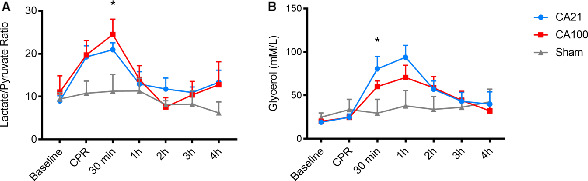
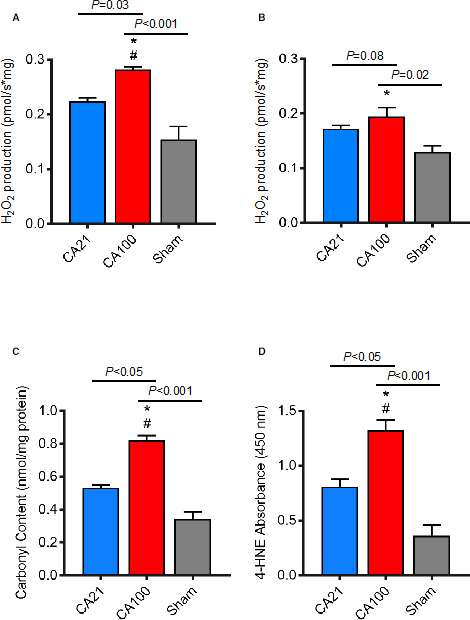
Background Hyperoxia during cardiopulmonary resuscitation (CPR) may lead to oxidative injury from mitochondrial-derived reactive oxygen species, despite guidelines recommending 1.0 inspired oxygen during CPR. We hypothesized exposure to 1.0 inspired oxygen during CPR would result in cerebral hyperoxia, higher mitochondrial-derived reactive oxygen species, increased oxidative injury, and similar survival compared with those exposed to 21% oxygen. Methods and Results Four-week-old piglets (n=25) underwent asphyxial cardiac arrest followed by randomization and blinding to CPR with 0.21 (n=10) or 1.0 inspired oxygen (n=10) through 10 minutes post return of spontaneous circulation. Sham was n=5. Survivors received 4 hours of protocolized postarrest care, whereupon brain was obtained for mitochondrial analysis and neuropathology. Groups were compared using Kruskal-Wallis test, Wilcoxon rank-sum test, and generalized estimating equations regression models. Both 1.0 and 0.21 groups were similar in systemic hemodynamics and cerebral blood flow, as well as survival (8/10). The 1.0 animals had relative cerebral hyperoxia during CPR and immediately following return of spontaneous circulation (brain tissue oxygen tension, 85% [interquartile range, 72%-120%] baseline in 0.21 animals versus 697% [interquartile range, 515%-721%] baseline in 1.0 animals; =0.001 at 10 minutes postarrest). Cerebral mitochondrial reactive oxygen species production was higher in animals treated with 1.0 compared with 0.21 (<0.03). Exposure to 1.0 oxygen led to increased cerebral oxidative injury to proteins and lipids, as evidenced by significantly higher protein carbonyls and 4-hydroxynoneals compared with 0.21 (<0.05) and sham (<0.001). Conclusions Exposure to 1.0 inspired oxygen during CPR caused cerebral hyperoxia during resuscitation, and resultant increased mitochondrial-derived reactive oxygen species and oxidative injury following cardiac arrest.
心肺复苏(CPR)期间的高氧可能会导致线粒体来源的活性氧引起氧化损伤,尽管指南建议 CPR 期间吸入 1.0 的氧气。我们假设在 CPR 期间暴露于 1.0 的吸入氧气会导致脑过度氧合、更高的线粒体来源的活性氧、增加的氧化损伤,并且与暴露于 21%氧气的患者相比具有相似的存活率。
4 周龄的小猪(n=25)经历窒息性心脏骤停,然后随机分配并在自主循环恢复后 10 分钟内接受 0.21(n=10)或 1.0 吸入氧气(n=10)的 CPR,进行盲法处理。假手术组 n=5。幸存者接受 4 小时的协议化复苏后护理,然后获取大脑进行线粒体分析和神经病理学检查。使用 Kruskal-Wallis 检验、Wilcoxon 秩和检验和广义估计方程回归模型比较各组。1.0 和 0.21 组在全身血流动力学和脑血流以及存活率方面相似(8/10)。1.0 组动物在 CPR 期间和自主循环恢复后立即出现相对脑过度氧合(脑组织氧张力,0.21 组的基础值为 85%[四分位距,72%-120%],1.0 组的基础值为 697%[四分位距,515%-721%];=0.001 在心脏骤停后 10 分钟)。与 0.21 相比,用 1.0 处理的动物的脑线粒体活性氧的产生更高(<0.03)。暴露于 1.0 氧气导致脑蛋白质和脂质的氧化损伤增加,这表现为蛋白质羰基和 4-羟基壬烯醛的水平显著高于 0.21(<0.05)和假手术组(<0.001)。
CPR 期间暴露于 1.0 的吸入氧气会导致复苏期间脑过度氧合,并导致心脏骤停后线粒体来源的活性氧和氧化损伤增加。