Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Center for Musculoskeletal Surgery (CMSC), Charité - Universitätsmedizin Berlin, Charitéplatz 1, 10117, Berlin, Germany.
Infection. 2020 Aug;48(4):559-568. doi: 10.1007/s15010-020-01435-2. Epub 2020 May 5.
Biofilm-active antibiotics are suggested to improve the outcome of implant-associated infections; however, their role in infections after spinal instrumentation is unclear. Therefore, we evaluated the outcome of patients with spinal implant-associated infections treated with and without biofilm-active antibiotics.
The probability of infection-free survival was estimated for treatment of spinal implant-associated infections with and without biofilm-active antibiotics using the Kaplan-Meier method; Cox proportional-hazards regression model was used to identify factors associated with treatment failure.
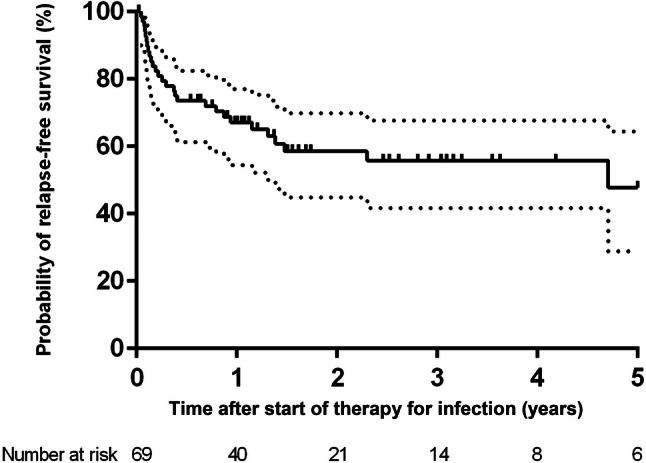
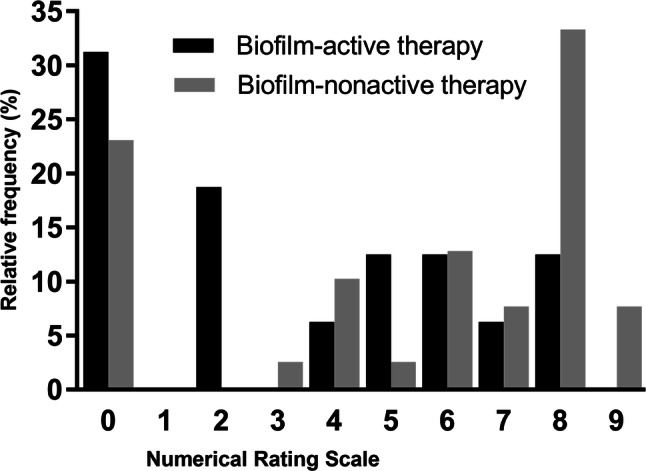
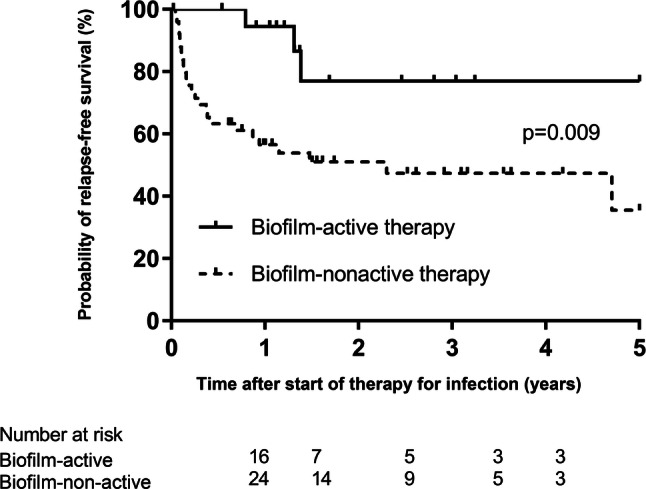
Among 93 included patients, early-onset infection was diagnosed in 61 (66%) and late-onset in 32 infections (34%). Thirty patients (32%) were treated with biofilm-active antibiotic therapy and 63 (68%) without it. The infection-free survival after a median follow-up of 53.7 months (range, 8 days-9.4 years) was 67% (95% confidence interval [CI], 55-82%) after 1 year and 58% (95% CI 43-71%) after 2 years. The infection-free survival after 1 and 2 years was 94% (95% CI 85-99%) and 84% (95% CI 71-93%) for patients treated with biofilm-active antibiotics, respectively, and 57% (95% CI 39-80%) and 49% (95% CI 28-61%) for those treated without biofilm-active antibiotics, respectively (p = 0.009). Treatment with biofilm-active antibiotics (hazard ratio [HR], 0.23, 95% CI 0.07-0.77), infection with Staphylococcus auras (HR, 2.19, 95% CI 1.04-4.62) and polymicrobial infection (HR, 2.44, 95% CI 1.09-6.04) were significantly associated with treatment outcome. Severe pain was observed more often in patients without biofilm-active antibiotic therapy (49% vs. 18%, p = 0.027).
Treatment with biofilm-active antibiotics was associated with better treatment outcome and less postoperative pain intensity.
生物膜活性抗生素被认为可以改善植入物相关感染的治疗效果;然而,其在脊柱器械相关感染中的作用尚不清楚。因此,我们评估了使用和不使用生物膜活性抗生素治疗脊柱植入物相关感染患者的结果。
使用 Kaplan-Meier 法估计生物膜活性抗生素治疗脊柱植入物相关感染的无感染生存概率;采用 Cox 比例风险回归模型确定与治疗失败相关的因素。
在 93 名纳入的患者中,61 名(66%)患者诊断为早期感染,32 名(34%)患者诊断为晚期感染。30 名(32%)患者接受了生物膜活性抗生素治疗,63 名(68%)患者未接受该治疗。在中位随访 53.7 个月(范围为 8 天至 9.4 年)后,1 年时无感染生存率为 67%(95%CI:55-82%),2 年时为 58%(95%CI:43-71%)。接受生物膜活性抗生素治疗的患者 1 年和 2 年的无感染生存率分别为 94%(95%CI:85-99%)和 84%(95%CI:71-93%),而未接受生物膜活性抗生素治疗的患者分别为 57%(95%CI:39-80%)和 49%(95%CI:28-61%)(p=0.009)。生物膜活性抗生素治疗(风险比[HR],0.23,95%CI:0.07-0.77)、金黄色葡萄球菌感染(HR,2.19,95%CI:1.04-4.62)和混合感染(HR,2.44,95%CI:1.09-6.04)与治疗结果显著相关。未接受生物膜活性抗生素治疗的患者中更常出现严重疼痛(49%比 18%,p=0.027)。
生物膜活性抗生素治疗与更好的治疗效果和术后疼痛强度降低相关。