Montreal Heart Institute, Université de Montréal, 5000 Belanger Street, Montréal, Québec H1T 1C8, Canada.
Université de Montpellier, INSERM, CNRS, CHU de Montpellier, Cardiology Department, CHU Arnaud de Villeneuve, 371, avenue du Doyen Gaston-Giraud, 34090 Montpellier, France.
Eur Heart J Qual Care Clin Outcomes. 2021 Sep 16;7(5):486-495. doi: 10.1093/ehjqcco/qcaa045.
In the randomized, placebo-controlled Colchicine Cardiovascular Outcomes Trial (COLCOT) of 4745 patients enrolled within 30 days after myocardial infarction (MI), low-dose colchicine (0.5 mg once daily) reduced the incidence of the primary composite endpoint of cardiovascular death, resuscitated cardiac arrest, MI, stroke, or urgent hospitalization for angina leading to coronary revascularization. To assess the in-trial period and lifetime cost-effectiveness of low-dose colchicine therapy compared to placebo in post-MI patients on standard-of-care therapy.
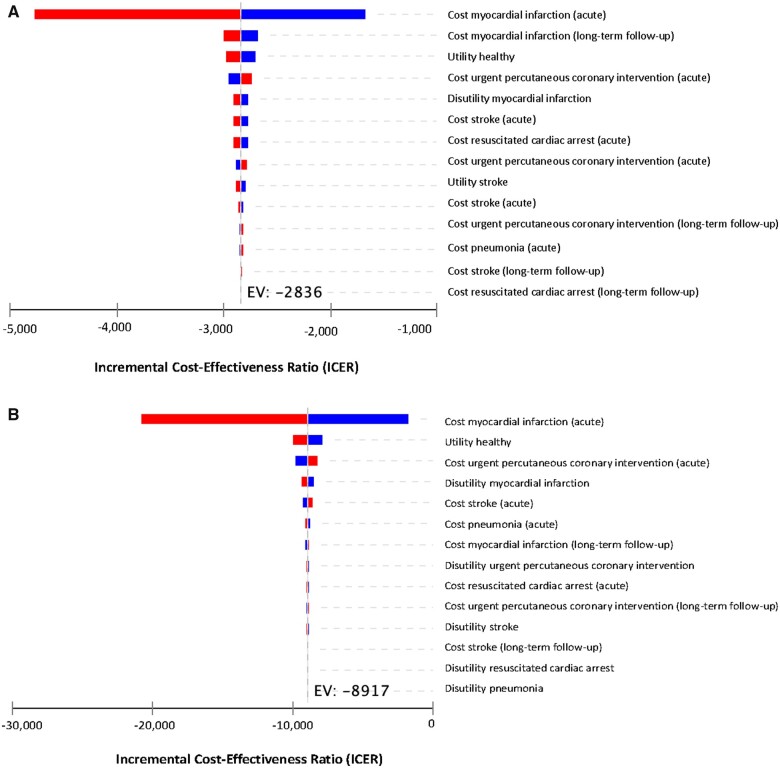
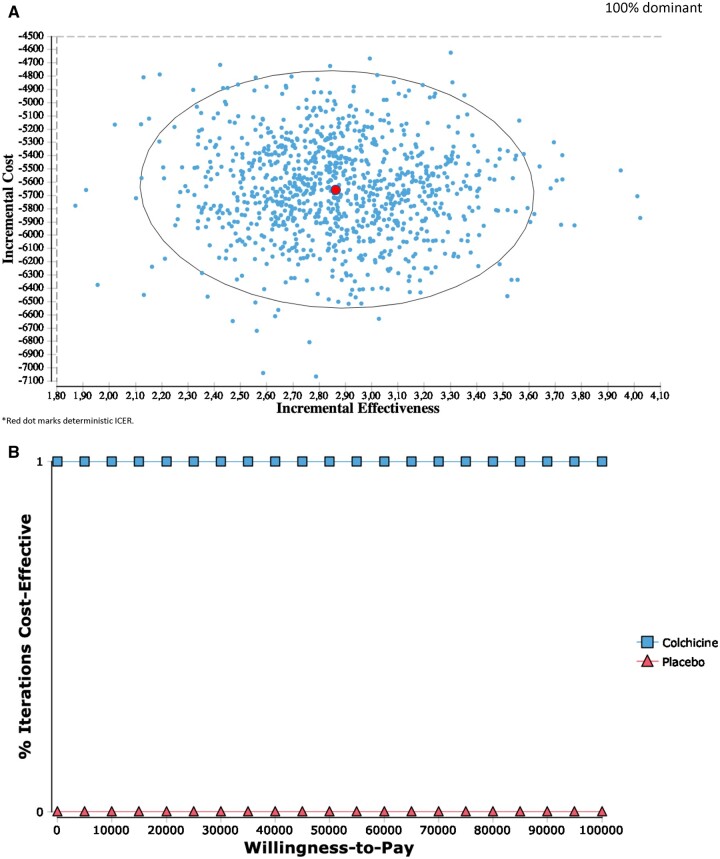
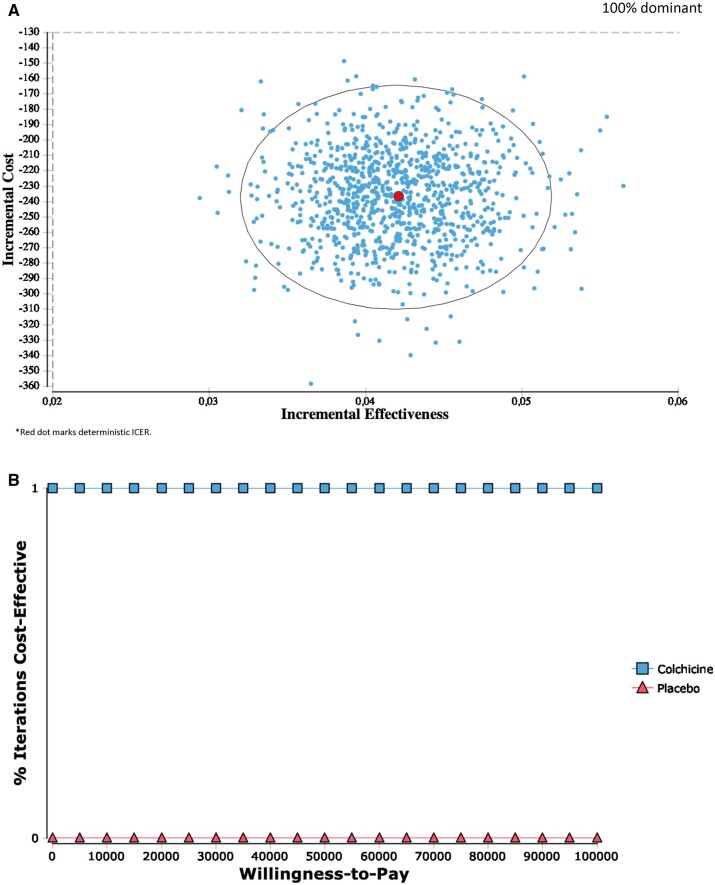
A multistate Markov model was developed incorporating the primary efficacy and safety results from COLCOT, as well as healthcare costs and utilities from the Canadian healthcare system perspective. All components of the primary outcome, non-cardiovascular deaths, and pneumonia were included as health states in the model as both primary and recurrent events. In the main analysis, a deterministic approach was used to estimate the incremental cost-effectiveness ratio (ICER) for the trial period (24 months) and lifetime (20 years). Over the in-trial period, the addition of colchicine to post-MI standard-of-care treatment decreased the mean overall per-patient costs by 47%, from $502 to $265 Canadian dollar (CAD), and increased the quality-adjusted life years (QALYs) from 1.30 to 1.34. The lifetime per-patient costs were further reduced (69%) and QALYs increased with colchicine therapy (from 8.82 to 11.68). As a result, both in-trial and lifetime ICERs indicated colchicine therapy was a dominant strategy.
Cost-effectiveness analyses indicate that the addition of colchicine to standard-of-care therapy after MI is economically dominant and therefore generates cost savings.
在纳入心肌梗死后 30 天内的 4745 例患者的随机、安慰剂对照的秋水仙碱心血管结局试验(COLCOT)中,小剂量秋水仙碱(0.5mg 每日 1 次)降低了主要复合终点的发生率,该终点包括心血管死亡、复苏性心脏骤停、心肌梗死、卒中和因心绞痛紧急住院行冠状动脉血运重建。评估 MI 后接受标准治疗的患者中,与安慰剂相比,小剂量秋水仙碱治疗的试验期间和终生成本效益。
采用多状态马尔可夫模型,纳入 COLCOT 的主要疗效和安全性结果,以及从加拿大医疗保健系统角度的医疗保健成本和效用。模型中的健康状态包括主要结局、非心血管死亡和肺炎,以及所有主要结局的组成部分,都是原发性和复发性事件。在主要分析中,采用确定性方法估算试验期间(24 个月)和终生(20 年)的增量成本效益比(ICER)。在试验期间,秋水仙碱联合 MI 标准治疗可降低每位患者的平均总费用 47%,从 502 加元降至 265 加元,并且提高质量调整生命年(QALY)从 1.30 至 1.34。进一步降低了终生每位患者的费用(69%),并增加了秋水仙碱治疗的 QALY(从 8.82 至 11.68)。因此,试验期间和终生的 ICER 均表明,秋水仙碱联合标准治疗是一种优势策略。
成本效益分析表明,MI 后联合标准治疗使用秋水仙碱具有经济优势,因此可节省成本。