Division of Anaesthesia, Addenbrooke's Hospital, University of Cambridge, Cambridge, UK.
Department of Surgery, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, MB, R3A 1R9, Canada.
J Clin Monit Comput. 2021 Aug;35(4):711-722. doi: 10.1007/s10877-020-00527-6. Epub 2020 May 16.
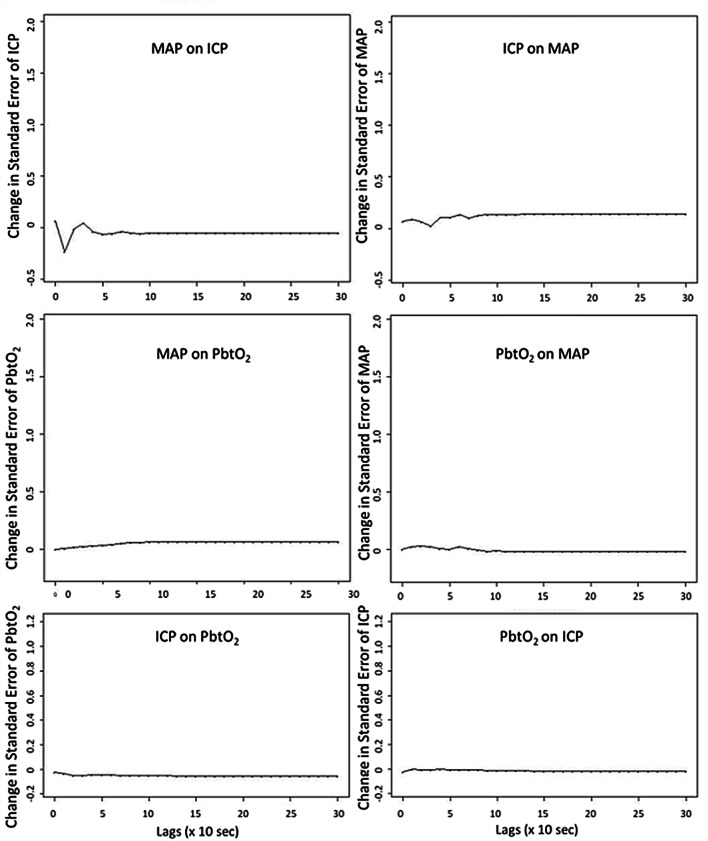
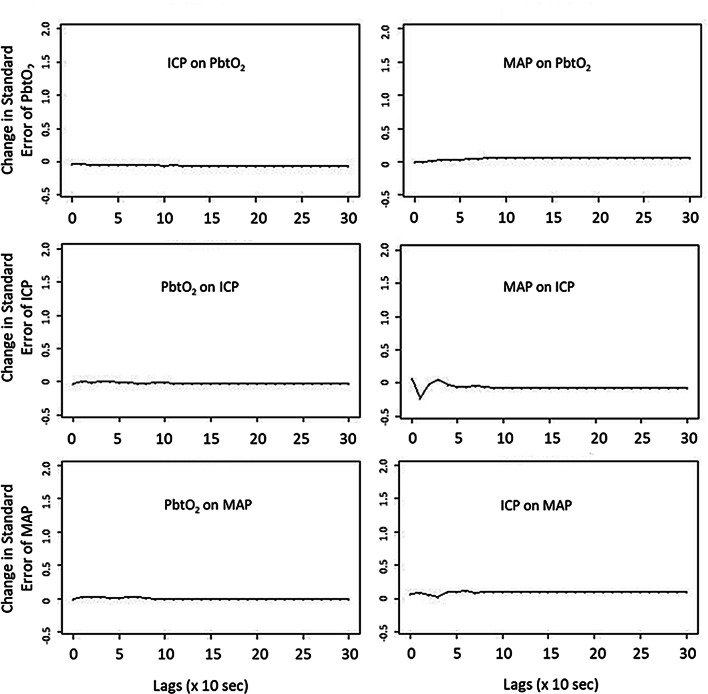
Brain tissue oxygen (PbtO) monitoring in traumatic brain injury (TBI) has demonstrated strong associations with global outcome. Additionally, PbtO signals have been used to derive indices thought to be associated with cerebrovascular reactivity in TBI. However, their true relationship to slow-wave vasogenic fluctuations associated with cerebral autoregulation remains unclear. The goal of this study was to investigate the relationship between slow-wave fluctuations of intracranial pressure (ICP), mean arterial pressure (MAP) and PbtO over time. Using the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) high resolution ICU sub-study cohort, we evaluated those patients with recorded high-frequency digital intra-parenchymal ICP and PbtO monitoring data of a minimum of 6 h in duration. Digital physiologic signals were processed for ICP, MAP, and PbtO slow-waves using a moving average filter to decimate the high-frequency signal. The first 5 days of recording were analyzed. The relationship between ICP, MAP and PbtO slow-waves over time were assessed using autoregressive integrative moving average (ARIMA) and vector autoregressive integrative moving average (VARIMA) modelling, as well as Granger causality testing. A total of 47 patients were included. The ARIMA structure of ICP and MAP were similar in time, where PbtO displayed different optimal structure. VARIMA modelling and IRF plots confirmed the strong directional relationship between MAP and ICP, demonstrating an ICP response to MAP impulse. PbtO slow-waves, however, failed to demonstrate a definite response to ICP and MAP slow-wave impulses. These results raise questions as to the utility of PbtO in the derivation of cerebrovascular reactivity measures in TBI. There is a reproducible relationship between slow-wave fluctuations of ICP and MAP, as demonstrated across various time-series analytic techniques. PbtO does not appear to reliably respond in time to slow-wave fluctuations in MAP, as demonstrated on various VARIMA models across all patients. These findings suggest that PbtO should not be utilized in the derivation of cerebrovascular reactivity metrics in TBI, as it does not appear to be responsive to changes in MAP in the slow-waves. These findings corroborate previous results regarding PbtO based cerebrovascular reactivity indices.
脑氧(PbtO)监测在创伤性脑损伤(TBI)中已被证明与整体预后有很强的相关性。此外,PbtO 信号已被用于推导被认为与 TBI 中脑血管反应性相关的指数。然而,它们与与脑自动调节相关的慢波血管源性波动的真正关系仍不清楚。本研究的目的是探讨颅内压(ICP)、平均动脉压(MAP)和 PbtO 随时间的慢波变化之间的关系。使用协作欧洲神经创伤效力研究在创伤性脑损伤(CENTER-TBI)高分辨率 ICU 子研究队列中,我们评估了那些记录有至少 6 小时高频率数字脑室内 ICP 和 PbtO 监测数据的患者。使用移动平均滤波器对数字生理信号进行 ICP、MAP 和 PbtO 慢波处理,以对高频信号进行细化。分析了记录的前 5 天。使用自回归综合移动平均(ARIMA)和向量自回归综合移动平均(VARIMA)模型以及格兰杰因果关系检验评估了 ICP、MAP 和 PbtO 慢波随时间的关系。共纳入 47 例患者。ARIMA 结构在时间上,ICP 和 MAP 相似,而 PbtO 显示出不同的最佳结构。VARIMA 模型和 IRF 图证实了 MAP 和 ICP 之间的强烈方向关系,表明 ICP 对 MAP 脉冲的响应。然而,PbtO 慢波未能对 ICP 和 MAP 慢波脉冲表现出明确的反应。这些结果引发了关于 PbtO 在 TBI 中推导脑血管反应性测量的实用性的问题。在各种时间序列分析技术中,已经证明了 ICP 和 MAP 慢波波动之间存在可重复的关系。在所有患者的各种 VARIMA 模型上,PbtO 似乎都不能可靠地对 MAP 的慢波波动及时做出反应。这些发现表明,在 TBI 中推导脑血管反应性指标时不应该使用 PbtO,因为它似乎对 MAP 在慢波中的变化没有反应。这些发现与之前关于基于 PbtO 的脑血管反应性指数的结果相吻合。