Buder Anna, Hochmair Maximilian J, Setinek Ulrike, Pirker Robert, Filipits Martin
Institute of Cancer Research, Department of Medicine I, Comprehensive Cancer Center, Medical University of Vienna, Vienna, Austria.
Karl Landsteiner Institute of Lung Research and Pulmonary Oncology, Department of Respiratory and Critical Care Medicine, Hospital North, Vienna, Austria.
Transl Lung Cancer Res. 2020 Apr;9(2):239-245. doi: 10.21037/tlcr.2020.03.02.
Osimertinib has become standard therapy of advanced epidermal growth factor receptor ()-mutated non-small cell lung cancer (NSCLC) patients and T790M-mediated resistance. We investigated the clinical utility of mutation tracking in plasma-based circulating tumor DNA (ctDNA) after start of osimertinib therapy in metastatic, -mutant NSCLC patients who had progressed on prior therapy with EGFR tyrosine kinase inhibitors (TKIs).
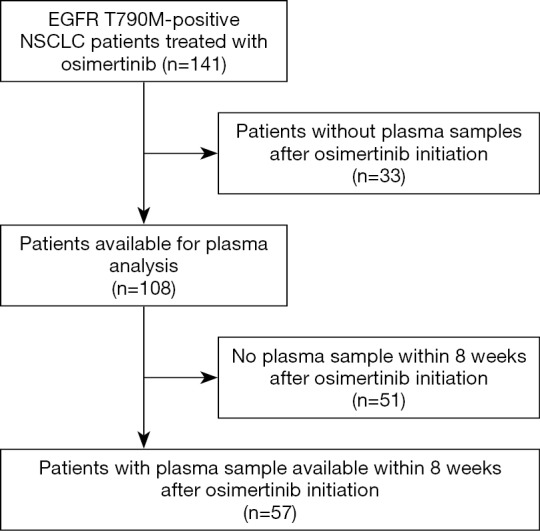
We enrolled 141 patients with advanced -mutated NSCLC who underwent second-line osimertinib treatment for T790M-positive disease. After initiation of osimertinib, we obtained plasma samples from 108 patients. Plasma ctDNA was tested for mutations by means of droplet digital PCR and was termed positive if any mutation was detected.
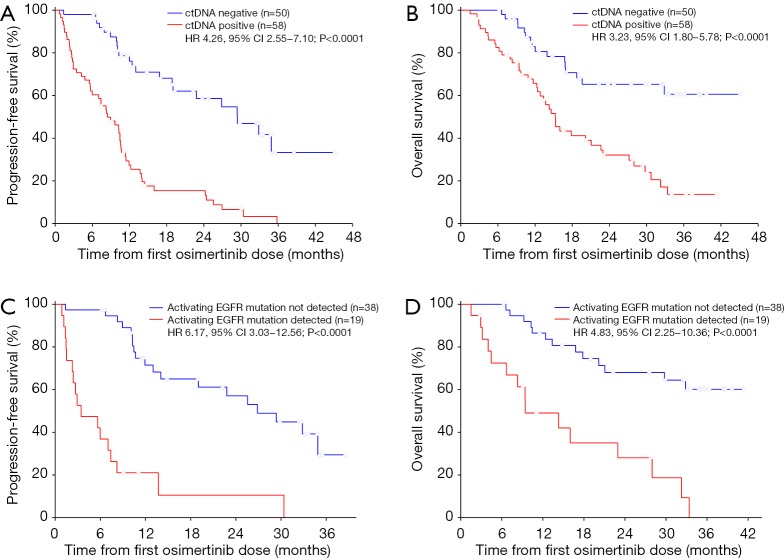
Plasma ctDNA was detected in 58 of 108 (54%) patients after osimertinib initiation and was associated with poor progression-free survival (PFS) [hazard ratio (HR) 4.26, 95% confidence interval (CI): 2.55-7.10, P<0.0001] and overall survival (OS) (HR 3.23, 95% CI: 1.80-5.78, P<0.0001). In multivariable analysis, ctDNA status remained significantly associated with PFS and OS (HR 4.87, 95% CI: 2.81-8.44, P<0.0001; HR 3.49, 95% CI: 1.88-6.50, P<0.0001). Patients with persistence of activating EGFR mutations within eight weeks had shorter durations of PFS (HR 6.17, 95% CI: 3.03-12.56, P<0.0001) and OS (HR 4.83, 95% CI: 2.25-10.36, P<0.0001) than patients with total clearance of the activating EGFR mutation. Persistence of activating EGFR mutations in plasma ctDNA remained an independent predictor of poor PFS and OS in multivariable analyses.
Patients with persistence of activating mutations in plasma ctDNA within eight weeks after osimertinib initiation have worse prognosis and may require the addition of chemotherapy or other treatments in order to achieve better outcome.
奥希替尼已成为晚期表皮生长因子受体(EGFR)突变的非小细胞肺癌(NSCLC)患者及T790M介导的耐药的标准治疗方案。我们研究了在接受奥希替尼治疗后,转移性、EGFR突变的NSCLC患者中,基于血浆的循环肿瘤DNA(ctDNA)中EGFR突变追踪的临床应用价值,这些患者在既往接受EGFR酪氨酸激酶抑制剂(TKIs)治疗时病情进展。
我们纳入了141例晚期EGFR突变的NSCLC患者,他们因T790M阳性疾病接受二线奥希替尼治疗。奥希替尼开始治疗后,我们从108例患者中获取了血浆样本。通过液滴数字PCR检测血浆ctDNA中的EGFR突变,若检测到任何EGFR突变,则判定为阳性。
奥希替尼开始治疗后,108例患者中有58例(54%)检测到血浆ctDNA,其与无进展生存期(PFS)较差相关[风险比(HR)4.26,95%置信区间(CI):2.55 - 7.10,P<0.0001],与总生存期(OS)也较差相关(HR 3.23,95% CI:1.80 - 5.78,P<0.0001)。在多变量分析中,ctDNA状态仍与PFS和OS显著相关(HR 4.87,95% CI:2.81 - 8.44,P<0.0001;HR 3.49,95% CI:1.88 - 6.50,P<0.0001)。在8周内持续存在激活型EGFR突变的患者,其PFS(HR 6.17,95% CI:3.03 - 12.56,P<0.0001)和OS(HR 4.83,95% CI:2.25 - 10.36,P<0.0001)的持续时间比激活型EGFR突变完全清除的患者短。血浆ctDNA中激活型EGFR突变的持续存在,在多变量分析中仍是PFS和OS较差的独立预测因素。
奥希替尼开始治疗后8周内,血浆ctDNA中持续存在激活型EGFR突变的患者预后较差,可能需要加用化疗或其他治疗以获得更好的疗效。