Center for Global Infectious Disease Research, Seattle Children's Research Institute, Seattle, WA, United States.
Department of Obstetrics & Gynecology, University of Washington, Seattle, WA, United States.
Front Immunol. 2020 Apr 30;11:770. doi: 10.3389/fimmu.2020.00770. eCollection 2020.
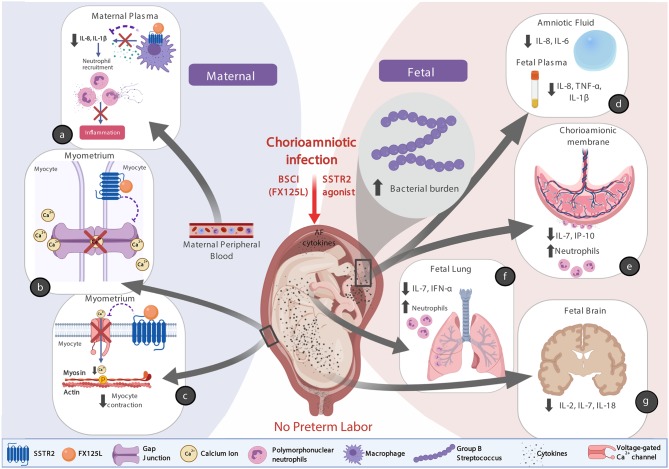
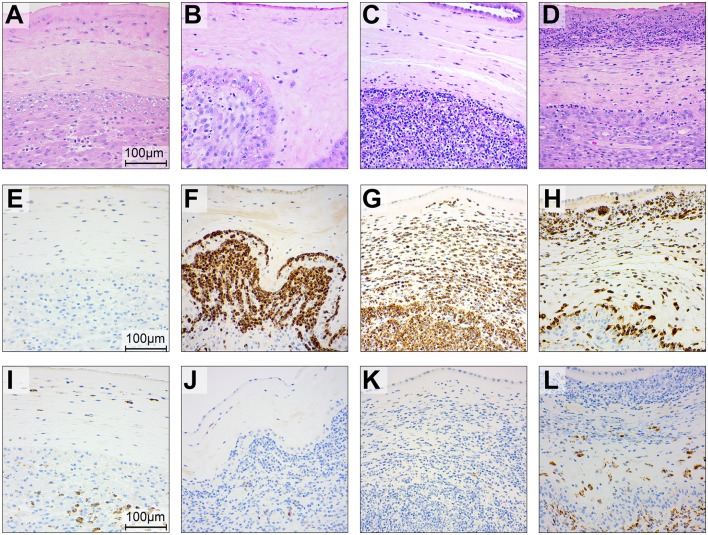
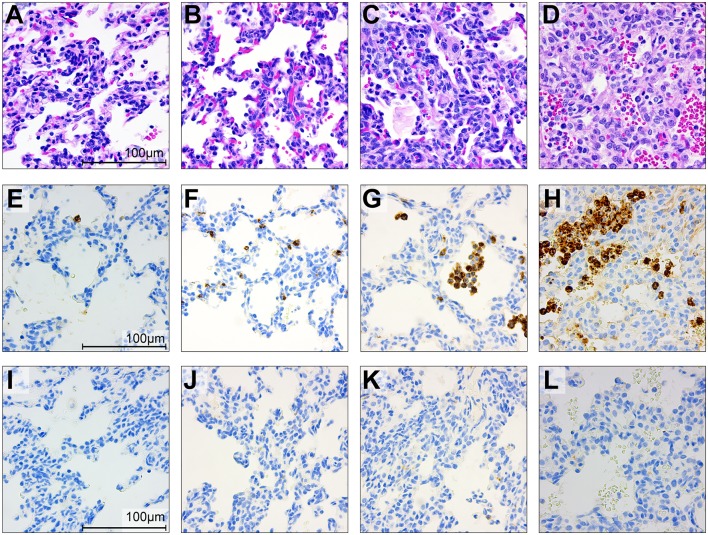
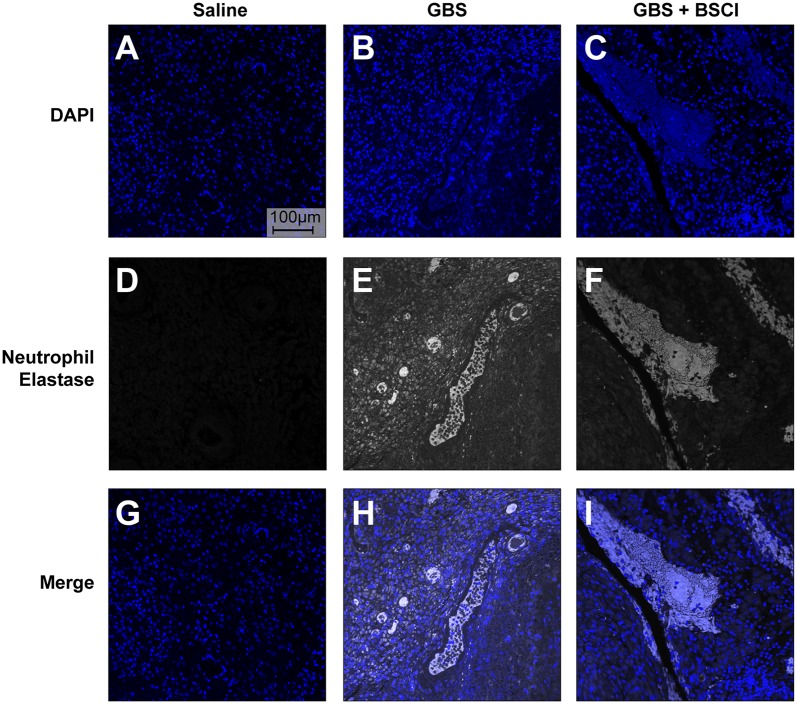
Leukocyte activation within the chorioamniotic membranes is strongly associated with inflammation and preterm labor (PTL). We hypothesized that prophylaxis with a broad-spectrum chemokine inhibitor (BSCI) would downregulate the inflammatory microenvironment induced by Group B Streptococcus (GBS, ) to suppress PTL and microbial invasion of the amniotic cavity (MIAC). To correlate BSCI administration with PTL and MIAC, we used a unique chronically catheterized non-human primate model of Group B Streptococcus (GBS)-induced PTL. In the early third trimester (128-138 days gestation; ~29-32 weeks human pregnancy), animals received choriodecidual inoculations of either: (1) saline ( = 6), (2) GBS, 1-5 × 10 colony forming units (CFU)/ml; = 5), or (3) pre-treatment and daily infusions of a BSCI (10 mg/kg intravenous and intra-amniotic) with GBS (1-5 × 10 CFU/ml; = 4). We measured amniotic cavity pressure (uterine contraction strength) and sampled amniotic fluid (AF) and maternal blood serially and cord blood at delivery. Cesarean section was performed 3 days post-inoculation or earlier for PTL. Data analysis used Fisher's exact test, Wilcoxon rank sum and one-way ANOVA with Bonferroni correction. Saline inoculation did not induce PTL or infectious sequelae. In contrast, GBS inoculation typically induced PTL (4/5, 80%), MIAC and fetal bacteremia (3/5; 60%). Remarkably, PTL did not occur in the BSCI+GBS group (0/4, 0%; = 0.02 vs. GBS), despite MIAC and fetal bacteremia in all cases (4/4; 100%). Compared to the GBS group, BSCI prophylaxis was associated with significantly lower cytokine levels including lower IL-8 in amniotic fluid ( = 0.03), TNF-α in fetal plasma ( < 0.05), IFN-α and IL-7 in the fetal lung ( = 0.02) and IL-18, IL-2, and IL-7 in the fetal brain ( = 0.03). Neutrophilic chorioamnionitis was common in the BSCI and GBS groups, but was more severe in the BSCI+GBS group with greater myeloperoxidase staining (granulocyte marker) in the amnion and chorion ( < 0.05 vs. GBS). Collectively, these observations indicate that blocking the chemokine response to infection powerfully suppressed uterine contractility, PTL and the cytokine response, but did not prevent MIAC and fetal pneumonia. Development of PTL immunotherapies should occur in tandem with evaluation for AF microbes and consideration for antibiotic therapy.
在羊膜绒毛膜中白细胞的激活与炎症和早产(PTL)密切相关。我们假设使用广谱趋化因子抑制剂(BSCI)进行预防,将下调由 B 群链球菌(GBS)引起的炎症微环境,以抑制 PTL 和微生物侵袭羊膜腔(MIAC)。为了将 BSCI 给药与 PTL 和 MIAC 相关联,我们使用了一种独特的慢性导管化非人灵长类动物模型,用于研究 GBS 诱导的 PTL。在妊娠晚期(128-138 天;约 29-32 周的人类妊娠),动物接受了绒毛膜蜕膜的以下三种处理:(1)生理盐水(=6),(2)GBS,1-5×10 个菌落形成单位(CFU)/ml;=5),或(3)GBS 前处理和每日 BSCI 输注(静脉内和羊膜内 10mg/kg)与 GBS(1-5×10 CFU/ml;=4)。我们连续测量羊膜腔压力(子宫收缩强度),并在分娩时采集羊水(AF)和母血以及脐带血。在接种后 3 天或更早进行剖宫产以预防 PTL。数据分析采用 Fisher 确切检验、Wilcoxon 秩和检验和单因素方差分析,采用 Bonferroni 校正。生理盐水接种不会引起 PTL 或感染性后遗症。相反,GBS 接种通常会引起 PTL(4/5,80%)、MIAC 和胎儿菌血症(3/5;60%)。值得注意的是,BSCI+GBS 组未发生 PTL(0/4,0%;=0.02 与 GBS 相比),尽管所有病例均发生 MIAC 和胎儿菌血症(4/4;100%)。与 GBS 组相比,BSCI 预防与明显较低的细胞因子水平相关,包括羊水中的 IL-8 降低(=0.03)、胎儿血浆中的 TNF-α 降低(<0.05)、胎儿肺中的 IFN-α 和 IL-7 降低(=0.02)以及胎儿脑中的 IL-18、IL-2 和 IL-7 降低(=0.03)。BSCI 和 GBS 组中常见中性粒细胞性绒毛膜羊膜炎,但在 BSCI+GBS 组中更严重,羊膜和绒毛膜中的髓过氧化物酶染色(粒细胞标志物)更严重(<0.05 与 GBS 相比)。总的来说,这些观察结果表明,阻断趋化因子对感染的反应强烈抑制了子宫收缩性、PTL 和细胞因子反应,但不能预防 MIAC 和胎儿肺炎。PTL 免疫疗法的发展应与 AF 微生物的评估同时进行,并考虑抗生素治疗。