Kim Ju-Eun, Choi Dae-Jung, Park Eugene J
Department of Orthopedic Surgery, Himnaera Hospital, Busan, Korea.
Department of Orthopedic Surgery, Chungnam National University College of Medicine, Daejeon, Korea.
Asian Spine J. 2020 Dec;14(6):790-800. doi: 10.31616/asj.2019.0297. Epub 2020 May 21.
Here we perform a retrospective analysis regarding an incidental dural tear (IDT) during biportal endoscopic spinal surgery (BESS).
This study investigates the causes of IDT specifically related to technical procedures of BESS with the aim of lowering its risk during training.
The incidence of dural tear is reported 0.5%-18% in open spinal surgery and 1.7%-4.3% during endoscopic spinal surgery. Because conversion to open surgery for direct repair could become necessary during endoscopic spinal surgery, prevention of this complication is essential.
We have retrospectively studied IDTs by four surgeons during 1 or 2 years after starting BESS for lumbar degenerative diseases and analyzed the locations, sizes, and specific endoscopic conditions specific to each.
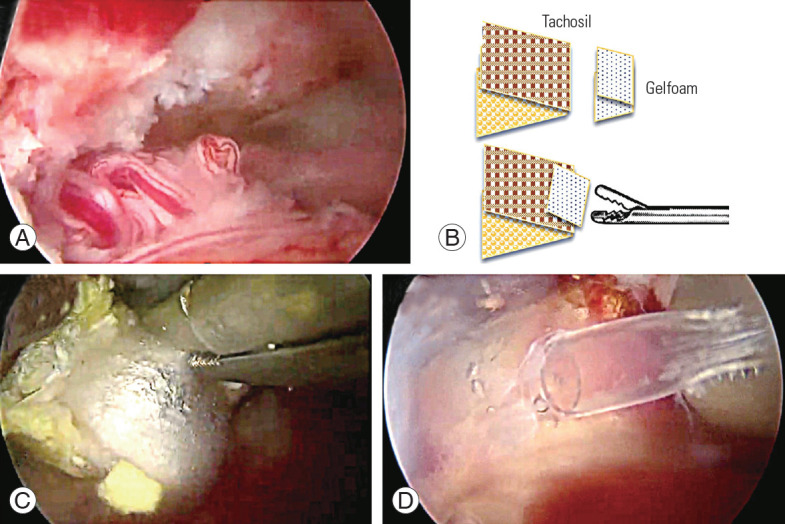
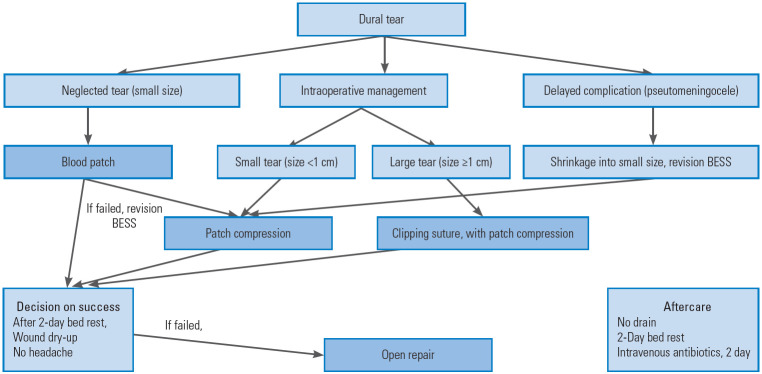
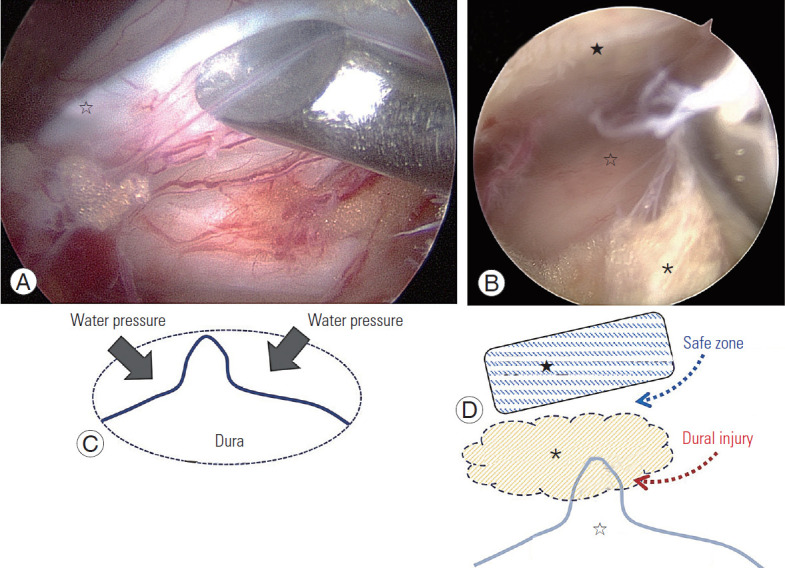
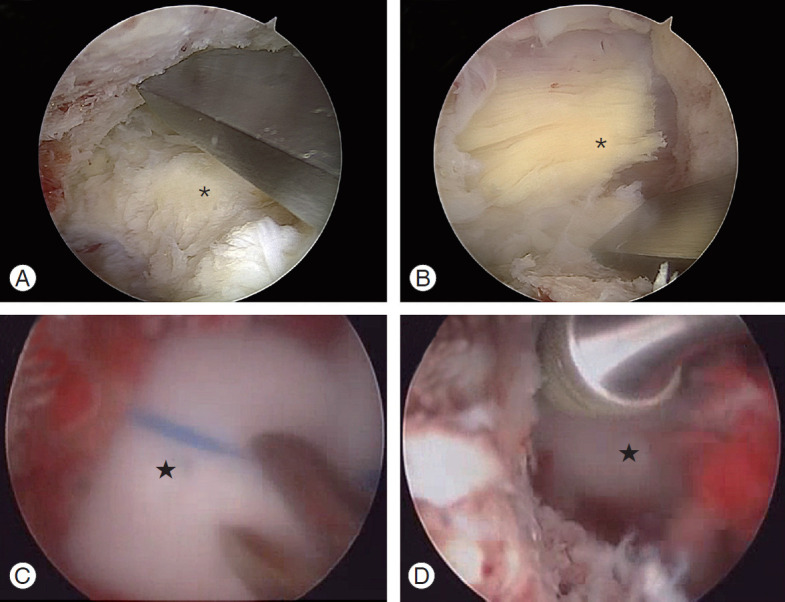
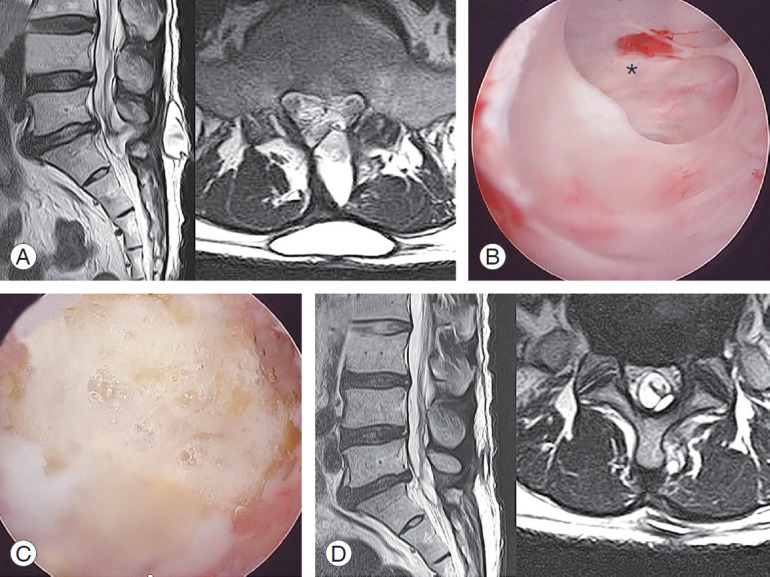
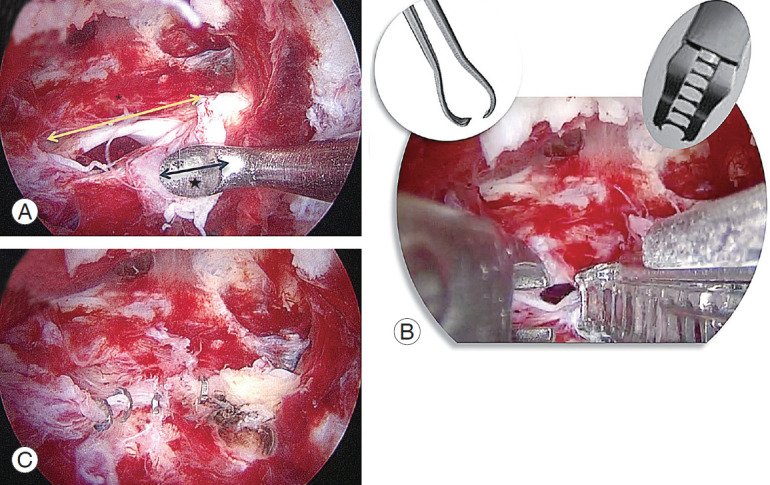
Twenty-five cases (1.6%) of IDTs among 1,551 cases of BESS occurred; 13 cases (52%) of these were within the first 6 months. The locations were dorsal midline in 12 cases, ipsilateral side in 11 cases, and contralateral side in two cases. The tear sizes were <10 mm in 20 cases and ≥10 mm in five cases. IDT commonly occurred due to injury of central dural folding during flavectomy under turbid surgical fields due to small bleeds under water. Twenty cases with IDTs of <10 mm were treated well with the patch technique. Among five cases of ≥10 mm, three underwent open repair within a few days, and two of these which failed to conservative management required a delayed revision operation due to pseudomeningocele. No cases progressed to surgical site infection or infectious spondylitis.
IDTs of <10 mm can be successfully treated with the patch technique. To prevent IDT during the early learning period, maintaining clear visibility by securing fluent saline outflow and meticulous hemostasis of small bleeding from exposed cancellous bone and epidural vessels is essential with caution not to injure the central dural folding during midline flavectomy.
在此我们对双门内镜脊柱手术(BESS)期间的意外硬脊膜撕裂(IDT)进行回顾性分析。
本研究调查与BESS技术操作具体相关的IDT原因,目的是在培训期间降低其风险。
据报道,开放脊柱手术中硬脊膜撕裂的发生率为0.5%-18%,内镜脊柱手术期间为1.7%-4.3%。由于在内镜脊柱手术期间可能需要转为开放手术进行直接修复,预防这种并发症至关重要。
我们对4位外科医生在开始进行BESS治疗腰椎退行性疾病后的1至2年内发生的IDT进行了回顾性研究,并分析了每例IDT的位置、大小和特定的内镜情况。
在1551例BESS病例中发生了25例(1.6%)IDT;其中13例(52%)发生在最初6个月内。位置在背侧中线的有12例,同侧的有11例,对侧的有2例。撕裂大小<10mm的有20例,≥10mm的有5例。IDT常见于在水下小出血导致手术视野浑浊的情况下进行黄韧带切除时中央硬脊膜折叠损伤。20例<10mm的IDT采用补片技术治疗效果良好。在5例≥10mm的病例中,3例在数天内接受了开放修复,其中2例保守治疗失败,因假性脑脊膜膨出需要延迟翻修手术。无病例进展为手术部位感染或感染性脊柱炎。
<10mm的IDT可通过补片技术成功治疗。为在早期学习阶段预防IDT,通过确保流畅的盐水流出保持清晰视野以及对暴露的松质骨和硬膜外血管的小出血进行细致止血至关重要,同时在中线黄韧带切除时要小心避免损伤中央硬脊膜折叠。