Anesthesia and Intensive Care, Ospedale Policlinico San Martino, IRCCS for Oncology and Neurosciences, Genoa, Italy.
Anesthesia and Intensive Care, Ospedale Policlinico San Martino, IRCCS for Oncology and Neurosciences, Genoa, Italy; Department of Surgical Sciences and Integrated Diagnostics, University of Genoa, Genoa, Italy.
Respir Physiol Neurobiol. 2020 Aug;279:103455. doi: 10.1016/j.resp.2020.103455. Epub 2020 May 11.
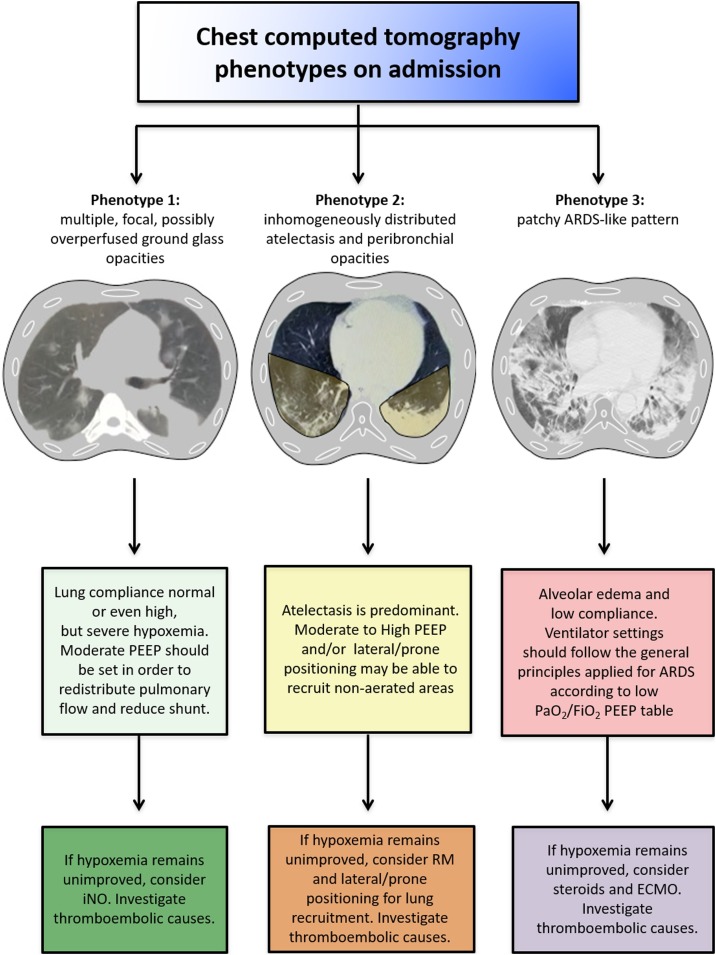
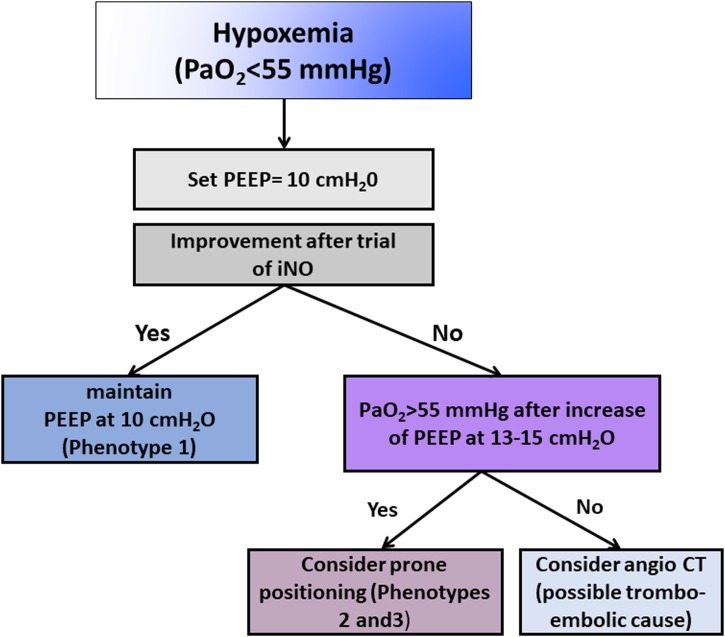
Coronavirus disease 2019 (COVID-19) can cause severe respiratory failure requiring mechanical ventilation. The abnormalities observed on chest computed tomography (CT) and the clinical presentation of COVID-19 patients are not always like those of typical acute respiratory distress syndrome (ARDS) and can change over time. This manuscript aimed to provide brief guidance for respiratory management of COVID-19 patients before, during, and after mechanical ventilation, based on the recent literature and on our direct experience with this population. We identify that chest CT patterns in COVID-19 may be divided into three main phenotypes: 1) multiple, focal, possibly overperfused ground-glass opacities; 2) inhomogeneously distributed atelectasis; and 3) a patchy, ARDS-like pattern. Each phenotype can benefit from different treatments and ventilator settings. Also, peripheral macro- and microemboli are common, and attention should be paid to the risk of pulmonary embolism. We suggest use of personalized mechanical ventilation strategies based on respiratory mechanics and chest CT patterns. Further research is warranted to confirm our hypothesis.
新型冠状病毒病(COVID-19)可导致需要机械通气的严重呼吸衰竭。COVID-19 患者的胸部计算机断层扫描(CT)异常表现和临床表现并不总是与典型的急性呼吸窘迫综合征(ARDS)一样,并且可能随时间而变化。本文旨在根据最近的文献和我们对该人群的直接经验,为 COVID-19 患者在机械通气前、中、后提供呼吸管理的简要指导。我们发现 COVID-19 的胸部 CT 模式可分为三种主要表型:1)多发、局灶性、可能过度灌注的磨玻璃影;2)分布不均的肺不张;3)斑片状、ARDS 样模式。每种表型都可以从不同的治疗和呼吸机设置中受益。此外,外周大栓子和微栓子很常见,应注意肺栓塞的风险。我们建议根据呼吸力学和胸部 CT 模式制定个性化的机械通气策略。需要进一步的研究来证实我们的假设。