Xu Yanling, Wang Qi, Meng Guangping, Li Dapeng, Ma Zhiming, Gao Peng, Zhang Jie, Zhang Qun, Su Zhenzhong
Department of Respiratory Medicine.
Department of Geriatrics and General Medicine.
Medicine (Baltimore). 2020 May;99(20):e20220. doi: 10.1097/MD.0000000000020220.
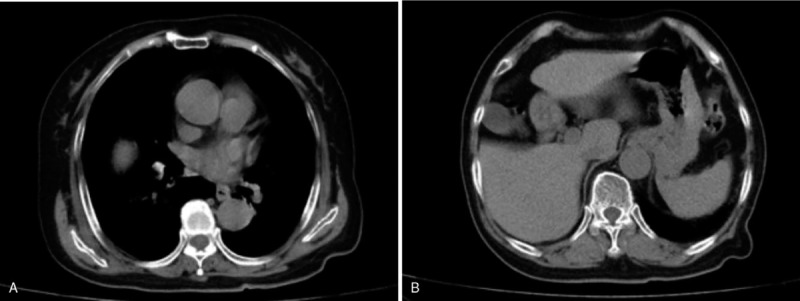
Chilaiditi syndrome is a rare disorder characterized by a broad spectrum of (gastro-intestinal) symptoms caused by interposition of a segment of bowel between the liver and the diaphragm. Most cases present with abdominal symptoms and the morbidity tend to increase with age.
Here we present a rare case of Chilaiditi syndrome. An elderly postmenopausal woman developed unresolved postoperative respiratory symptoms and chest pain. Chest auscultation revealed considerable attenuation of respiratory sounds. She showed postoperative increase in D-dimer level and sudden onset of dyspnea.
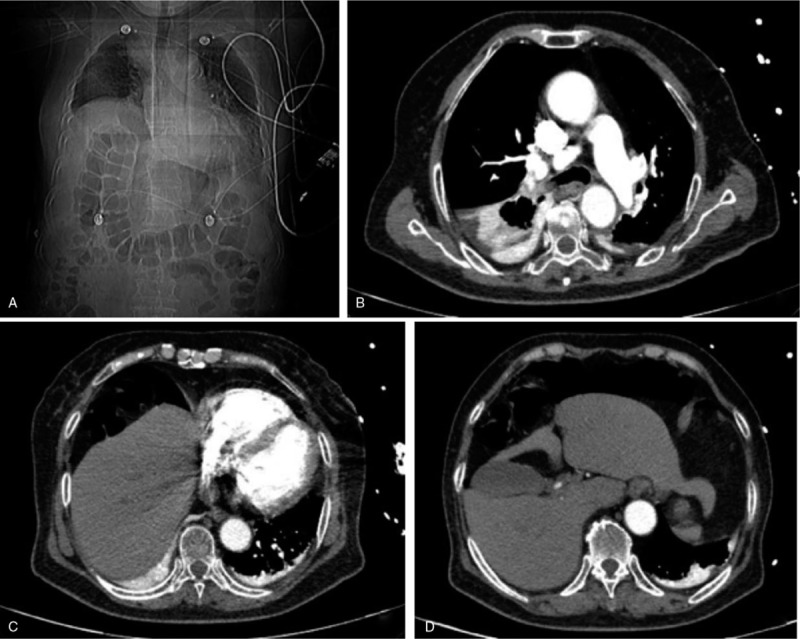
Considering the presence of atelectasis in the middle and lower lobes of the right lung, bedside fiberoptic bronchoscopy was performed immediately to rule out bronchial phlegm embolism. However, no phlegm embolism was found in the left lung, and a small amount of yellow-white mucus was seen in the upper lobe of the right lung. Due to external pressure, the lumen of the middle and lower lobes of the right lung was obviously narrowed.
The patient was placed in a semi-sitting position and a tube was passed through the anus to decompress the intestinal cavity; in addition, she received potassium supplementation.
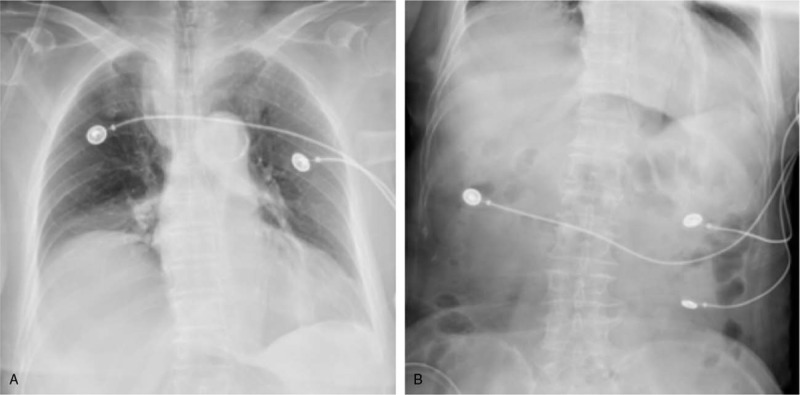
The patient's symptoms improved markedly. Chest and semi-supine abdominal plain radiographs showed enhanced lung markings, shadows in the left lower lung lobes, elevation of the right diaphragm, and small amount of pneumoperitoneum. The patient recovered after 5 days of continuous treatment and was discharged.
Emergency computed tomographic pulmonary angiography may facilitate the diagnosis of Chilaiditi syndrome, especially in the postoperative setting. Occurrence of Chilaiditi syndrome in this patient was likely associated with surgical factors. Appropriate investigations and clear identification of etiology are essential for successful treatment.
奇莱迪蒂综合征是一种罕见疾病,其特征为一段肠管位于肝脏与膈肌之间导致的一系列(胃肠道)症状。多数病例表现为腹部症状,且发病率往往随年龄增长而增加。
我们在此报告一例奇莱迪蒂综合征罕见病例。一位老年绝经后女性术后出现未缓解的呼吸道症状及胸痛。胸部听诊显示呼吸音明显减弱。她术后D - 二聚体水平升高且突然出现呼吸困难。
考虑到右肺中叶和下叶存在肺不张,立即进行床边纤维支气管镜检查以排除支气管痰栓形成。然而,左肺未发现痰栓,右肺上叶可见少量黄白色黏液。由于外部压迫,右肺中叶和下叶管腔明显变窄。
患者取半卧位,经肛门置管以减压肠腔;此外,给予补钾治疗。
患者症状明显改善。胸部及半卧位腹部平片显示肺纹理增强、左下肺叶有阴影、右膈抬高及少量气腹。经连续治疗5天后患者康复出院。
急诊计算机断层扫描肺动脉造影可能有助于奇莱迪蒂综合征的诊断,尤其是在术后情况。该患者奇莱迪蒂综合征的发生可能与手术因素有关。进行适当检查并明确病因对于成功治疗至关重要。