Department of Urology, The Affiliated Hospital of Qingdao University, Qingdao 266003, China.
Department of Special Inspection, Qingdao Eighth People's Hospital, Qingdao 266003, China.
Asian J Androl. 2021 Jan-Feb;23(1):41-46. doi: 10.4103/aja.aja_19_20.
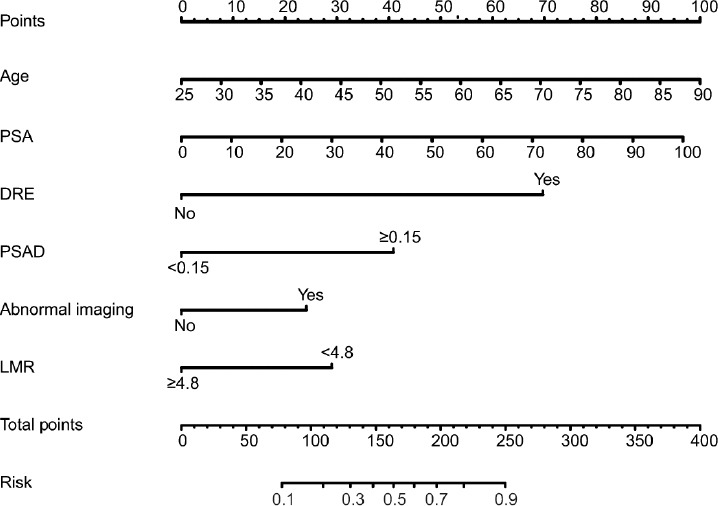
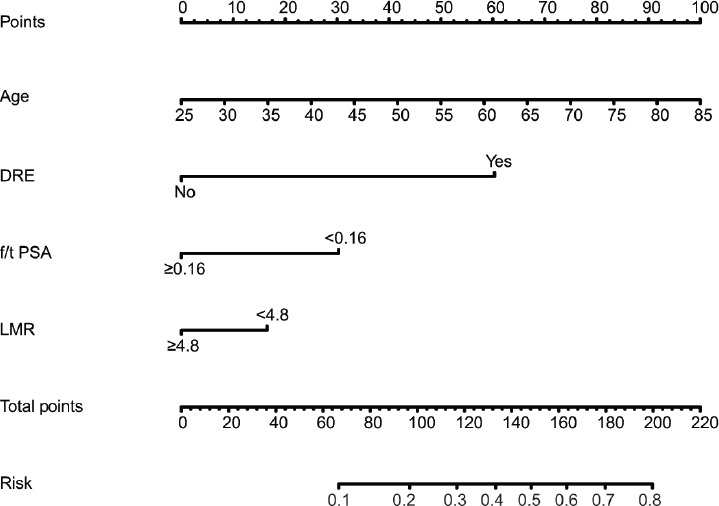
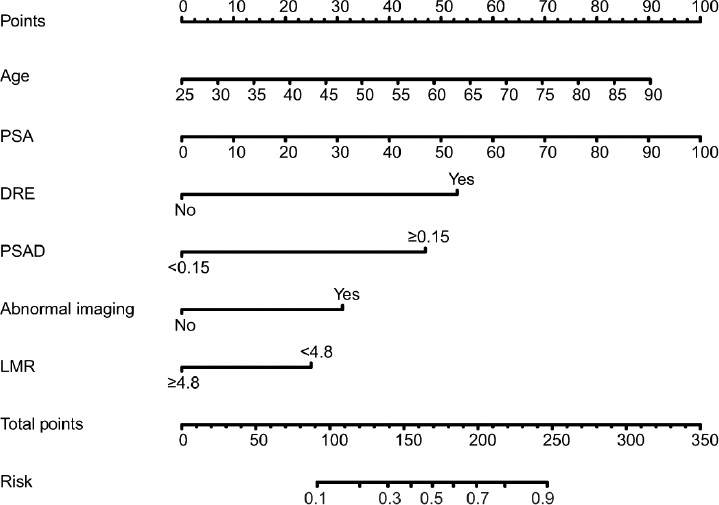
Here, we developed a prostate cancer (PCa) risk nomogram including lymphocyte-to-monocyte ratio (LMR) for initial prostate biopsy, and internal and external validation were further conducted. A prediction model was developed on a training set. Significant risk factors with P < 0.10 in multivariate logistic regression models were used to generate a nomogram. Discrimination, calibration, and clinical usefulness of the model were assessed using C-index, calibration plot, and decision curve analysis (DCA). The nomogram was re-examined with the internal and external validation set. A nomogram predicting PCa risk in patients with prostate-specific antigen (PSA) 4-10 ng ml was also developed. The model displayed good discrimination with C-index of 0.830 (95% confidence interval [CI]: 0.812-0.852). High C-index of 0.864 (95% CI: 0.840-0.888) and 0.871 (95% CI: 0.861-0.881) was still reached in the internal and external validation sets, respectively. The nomogram exhibited better performance compared to the nomogram with PSA only (C-index: 0.763, 95% CI: 0.746-0.780, P < 0.001) and the nomogram with LMR excluded (C-index: 0.824, 95% CI: 0.804-0.844, P < 0.010). The calibration curve demonstrated good agreement in the internal and external validation sets. DCA showed that the nomogram was useful at the threshold probability of >4% and <99%. The nomogram predicting PCa risk in patients with PSA 4-10 ng ml also displayed good calibration and discrimination performance (C-index: 0.734, 95% CI: 0.708-0.760). This nomogram incorporating age, PSA, digital rectal examination, abnormal imaging signals, PSA density, and LMR could be used to facilitate individual PCa risk prediction in initial prostate biopsy.
在这里,我们开发了一个包括淋巴细胞与单核细胞比值(LMR)在内的前列腺癌(PCa)风险列线图,用于初始前列腺活检,并进一步进行了内部和外部验证。在训练集中建立了预测模型。多变量逻辑回归模型中 P < 0.10 的显著风险因素用于生成列线图。使用 C 指数、校准图和决策曲线分析(DCA)评估模型的区分度、校准和临床实用性。该列线图在内部和外部验证集中进行了重新检查。还开发了一个预测前列腺特异性抗原(PSA)4-10ng/ml 患者 PCa 风险的列线图。该模型的区分度较好,C 指数为 0.830(95%置信区间[CI]:0.812-0.852)。内部和外部验证组的 C 指数分别为 0.864(95%CI:0.840-0.888)和 0.871(95%CI:0.861-0.881),仍然很高。与仅 PSA 的列线图(C 指数:0.763,95%CI:0.746-0.780,P < 0.001)和排除 LMR 的列线图(C 指数:0.824,95%CI:0.804-0.844,P < 0.010)相比,该列线图的性能更好。校准曲线在内部和外部验证组中均显示出良好的一致性。DCA 表明,该列线图在阈值概率>4%和<99%时是有用的。用于预测 PSA 4-10ng/ml 患者 PCa 风险的列线图也显示出良好的校准和区分性能(C 指数:0.734,95%CI:0.708-0.760)。该列线图纳入年龄、PSA、直肠指检、异常影像学信号、PSA 密度和 LMR,可用于辅助初始前列腺活检时个体 PCa 风险预测。