Benson Jessica R, Govindarajan Meinusha, Muir Jeffrey M, Lamb Iain R, Sculco Peter K
Department of Clinical Research, Intellijoint Surgical, Inc., Kitchener, Ontario, Canada.
Faculty of Applied Health Sciences, School of Public Health and Health Systems, University of Waterloo, Waterloo, Ontario, Canada.
Arthroplast Today. 2020 Jun 17;6(3):414-421. doi: 10.1016/j.artd.2020.04.003. eCollection 2020 Sep.
Changes in acetabular or hip center of rotation (HCOR) commonly occur during acetabular component preparation during total hip arthroplasty (THA). HCOR displacement in mediolateral or superoinferior directions is known to influence offset and leg length, but the incidence and range of HCOR change in the anteroposterior direction is less understood as the sagittal plane cannot be measured on standard anteroposterior radiographs. This study assessed the 3-dimensional displacement of HCOR after cup implantation and evaluated for potential factors associated with increased acetabular component translations.
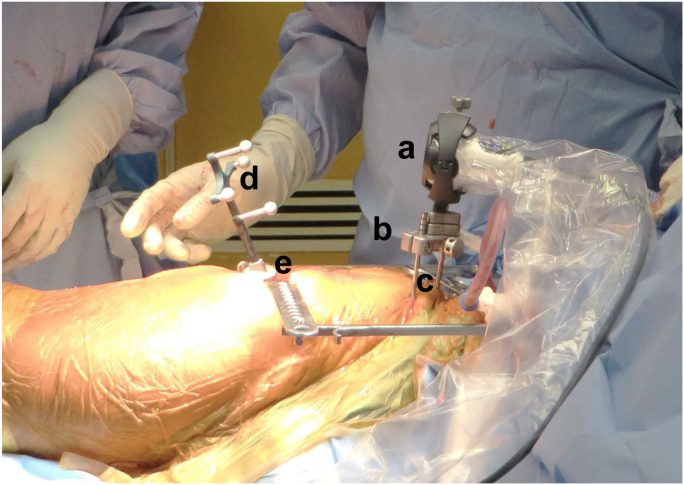
A total of 894 THAs were performed using a posterior, lateral, or direct anterior approach. Only intraoperative data from the navigation device were included in the analysis. All THAs performed between September 2015 and October 2017 were included. Paired tests were used to compare native HCOR and new HCOR values.
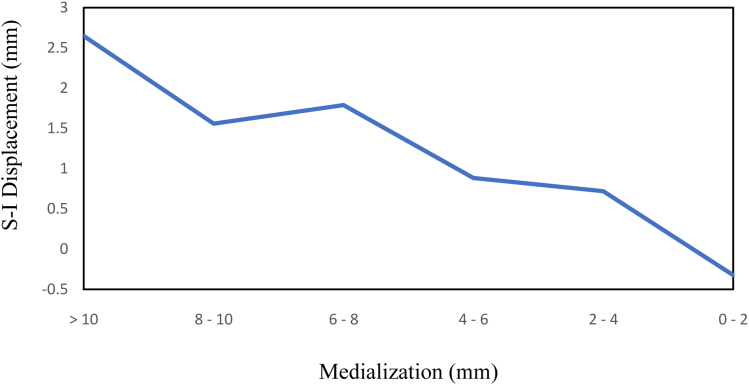
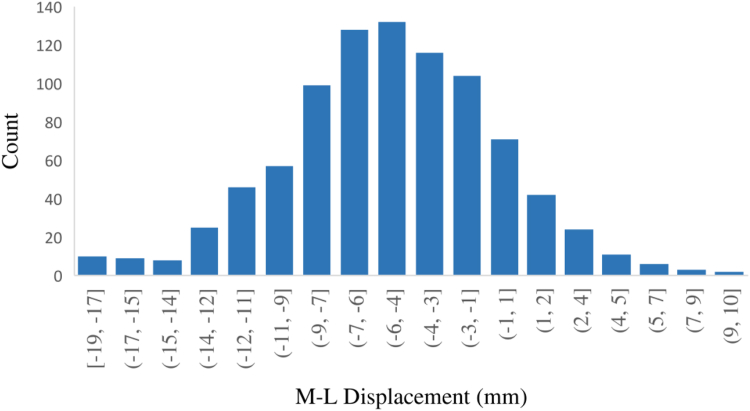
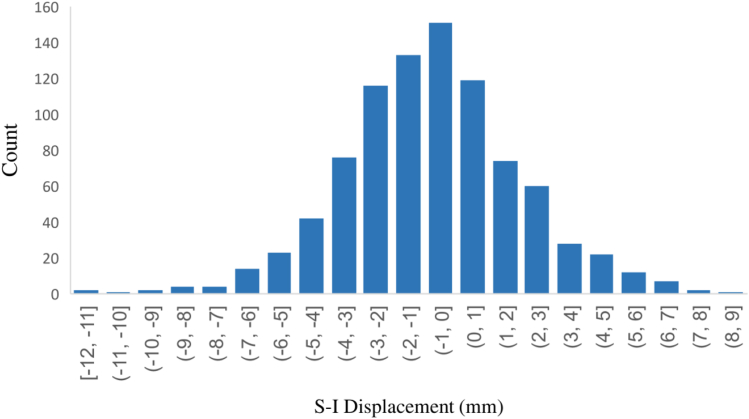
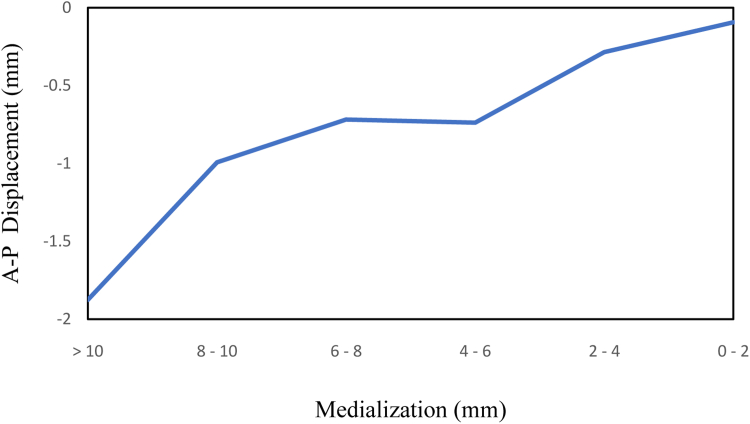
The mean HCOR displacement in 3 directions was 4.97mm medially ( < .001), 0.83mm superiorly ( < .001), and 0.64mm posteriorly ( < .001). Subgroup analysis revealed greater posterior HCOR displacement with the anterior approach than the lateral/posterior approach (2.32mm vs 0.44mm; < .001). Increasing medial HCOR displacement also resulted in increased superior and posterior HCOR displacement across surgical cases ( < .001).
HCOR displacement is commonly observed in medial, superior, and posterior directions. HCOR changes are influenced by surgical approach, potentially secondary to patient positioning, with greater posterior HCOR displacement observed in anterior cases. Surgeons should be aware of these factors, particularly in cases with deficient or reduced posterior column bone stock.
全髋关节置换术(THA)髋臼组件准备过程中,髋臼或髋关节旋转中心(HCOR)通常会发生变化。已知HCOR在内外侧或上下方向的位移会影响偏心距和肢体长度,但由于在标准前后位X线片上无法测量矢状面,因此对HCOR在前后方向变化的发生率和范围了解较少。本研究评估了髋臼杯植入后HCOR的三维位移,并评估了与髋臼组件平移增加相关的潜在因素。
采用后侧、外侧或直接前路进行了总共894例THA。分析仅纳入导航设备的术中数据。纳入2015年9月至2017年10月期间进行的所有THA。采用配对检验比较原始HCOR值和新的HCOR值。
HCOR在三个方向上的平均位移分别为:内侧4.97mm(P<0.001),上方0.83mm(P<0.001),后方0.64mm(P<0.001)。亚组分析显示,与外侧/后侧入路相比,前路手术的HCOR后移更大(2.32mm对0.44mm;P<0.001)。在所有手术病例中,HCOR内侧位移增加也导致HCOR上方和后方位移增加(P<0.001)。
HCOR位移常见于内侧、上方和后方。HCOR变化受手术入路影响,可能继发于患者体位,前路手术中HCOR后移更大。外科医生应了解这些因素,尤其是在后柱骨量不足或减少的病例中。