Department of Health Science, Clinica Pneumologica, AO San Gerardo, University of Milan Bicocca, Via Pergolesi 33, Monza, Italy.
BMC Pulm Med. 2014 Dec 5;14:194. doi: 10.1186/1471-2466-14-194.
To evaluate noninvasive ventilation (NIV) in diffuse interstitial lung diseases (DILD) patients with acute respiratory failure (ARF) according to baseline radiological patterns and the etiology of ARF.
In a multicenter, observational, retrospective study, consecutive DILD patients undergoing NIV because of an episode of ARF were evaluated in six Italian high dependency units. Three groups of patients were identified based on the etiology of ARF: those with pneumonia (Group A), those with acute exacerbation of fibrosis, (Group B) and those with other triggers (Group C). Clinical failure was defined as any among in-hospital mortality, endotracheal intubation and extra-corporeal membrane oxygenation use.
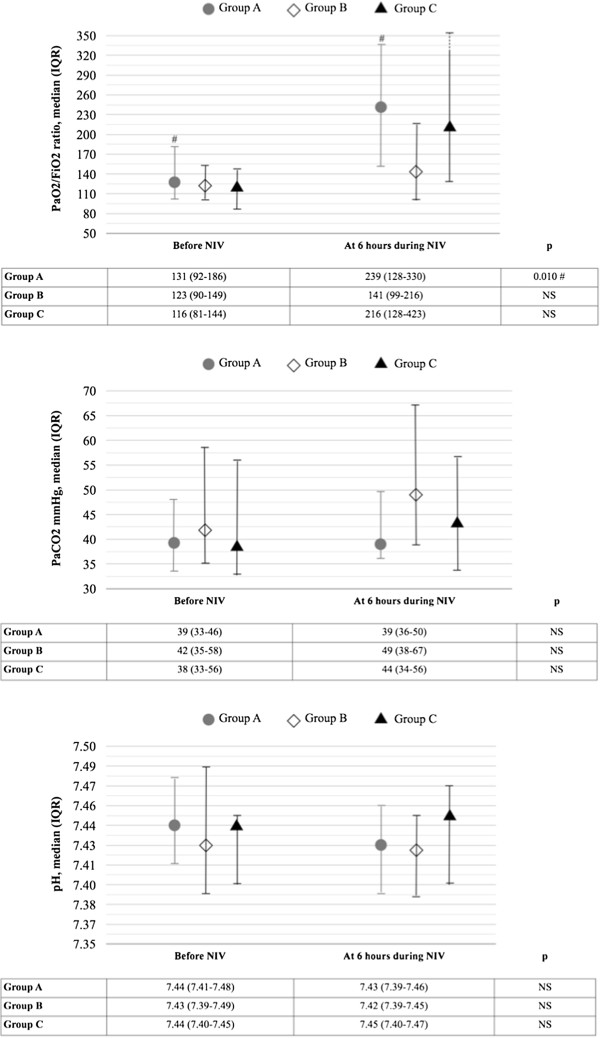
Among the 60 patients enrolled (63% males; median age: 71 years), pneumonia (42%) and acute exacerbation of fibrosis (39%) were the two most frequent causes of ARF. A significant increase of PaO2/FiO2 ratio during NIV treatment was detected in Group A (p = 0.010), but not in Group B. No significant difference in PaO2/FiO2 ratio, PaCO2 and pH values during NIV treatment was detected in patients with a radiological pattern of usual interstitial pneumonia (UIP) and non-specific interstitial pneumonia (NSIP). 22 patients (37%) suffered for a clinical failure. No significant differences in the study outcome were detected in Group A vs. Group B, as well as among patients with a radiological pattern of UIP vs.
NIV treatment should be individualized in DILD patients with ARF according to the etiology, but not the baseline radiological pattern, in order to improve oxygenation.
根据基线影像学模式和急性呼吸衰竭(ARF)的病因,评估弥漫性间质性肺疾病(DILD)患者的无创通气(NIV)。
在一项多中心、观察性、回顾性研究中,对六家意大利高依赖单位因 ARF 发作而接受 NIV 的连续 DILD 患者进行评估。根据 ARF 的病因将患者分为三组:肺炎(A 组)、纤维化急性加重(B 组)和其他诱因(C 组)。临床失败定义为住院死亡率、气管插管和体外膜氧合使用中的任何一种。
在纳入的 60 例患者中(63%为男性;中位年龄:71 岁),肺炎(42%)和纤维化急性加重(39%)是 ARF 的两个最常见原因。在 A 组中,NIV 治疗期间 PaO2/FiO2 比值显著增加(p = 0.010),但在 B 组中没有。在 UIP 和非特异性间质性肺炎(NSIP)的影像学模式中,NIV 治疗期间 PaO2/FiO2 比值、PaCO2 和 pH 值无显著差异。22 例(37%)患者临床失败。在 A 组与 B 组、UIP 与 NSIP 影像学模式的患者之间,研究结果无显著差异。
根据病因而非基线影像学模式,应个体化 DILD 患者的 NIV 治疗,以改善氧合。