Ferrandis Raquel, Llau Juan V, Sanz Javier F, Cassinello Concepción M, González-Larrocha Óscar, Matoses Salomé M, Suárez Vanessa, Guilabert Patricia, Torres Luís-Miguel, Fernández-Bañuls Esperanza, García-Cebrián Consuelo, Sierra Pilar, Barquero Marta, Montón Nuria, Martínez-Escribano Cristina, Llácer Manuel, Gómez-Luque Aurelio, Martín Julia, Hidalgo Francisco, Yanes Gabriel, Rodríguez Rubén, Castaño Beatriz, Duro Elena, Tapia Blanca, Pérez Antoni, Villanueva Ángeles M, Álvarez Juan-Carlos, Sabaté Sergi
Anaesthesiology and Critical Care, Hospital Universitari i Politècnic La Fe, València, Spain.
Anaesthesiology and Critical Care, Hospital Universitario Doctor Peset, València, Spain.
TH Open. 2020 Jun 26;4(2):e127-e137. doi: 10.1055/s-0040-1712476. eCollection 2020 Apr.
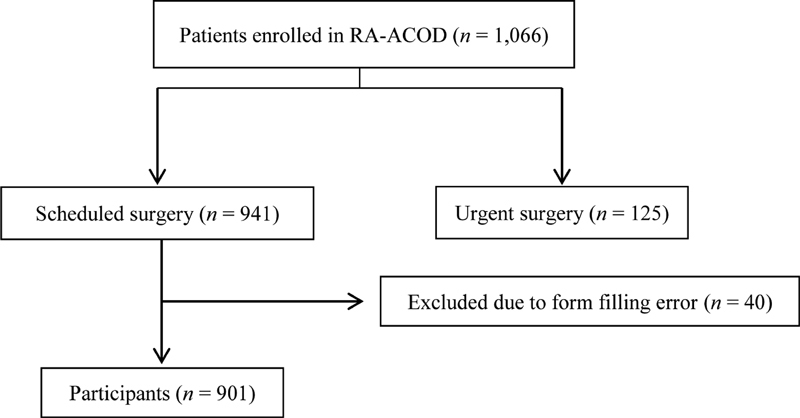
There is scarce real-world experience regarding direct oral anticoagulants (DOACs) perioperative management. No study before has linked bridging therapy or DOAC-free time (pre-plus postoperative time without DOAC) with outcome. The aim of this study was to investigate real-world management and outcomes. RA-ACOD is a prospective, observational, multicenter registry of adult patients on DOAC treatment requiring surgery. Primary outcomes were thrombotic and hemorrhagic complications. Follow-up was immediate postoperative (24-48 hours) and 30 days. Statistics were performed using a univariate and multivariate analysis. Data are presented as odds ratios (ORs [95% confidence interval]). From 26 Spanish hospitals, 901 patients were analyzed (53.5% major surgeries): 322 on apixaban, 304 on rivaroxaban, 267 on dabigatran, 8 on edoxaban. Fourteen (1.6%) patients suffered a thrombotic event, related to preoperative DOAC withdrawal (OR: 1.57 [1.03-2.4]) and DOAC-free time longer than 6 days (OR: 5.42 [1.18-26]). Minor bleeding events were described in 76 (8.4%) patients, with higher incidence for dabigatran (12.7%) versus other DOACs (6.6%). Major bleeding events occurred in 17 (1.9%) patients. Bridging therapy was used in 315 (35%) patients. It was associated with minor (OR: 2.57 [1.3-5.07]) and major (OR: 4.2 [1.4-12.3]) bleeding events, without decreasing thrombotic events. This study offers real-world data on perioperative DOAC management and outcomes in a large prospective sample size to date with a high percentage of major surgery. Short-term preprocedural DOAC interruption depending on the drug, hemorrhagic risk, and renal function, without bridging therapy and a reduced DOAC-free time, seems the safest practice.
关于直接口服抗凝剂(DOACs)围手术期管理,几乎没有真实世界的经验。此前没有研究将桥接治疗或无DOAC时间(术前加术后无DOAC的时间)与预后联系起来。本研究的目的是调查真实世界的管理情况和预后。RA - ACOD是一项针对接受DOAC治疗且需要手术的成年患者的前瞻性、观察性、多中心注册研究。主要结局是血栓形成和出血并发症。随访在术后即刻(24 - 48小时)和30天进行。采用单变量和多变量分析进行统计。数据以比值比(ORs [95%置信区间])表示。来自26家西班牙医院的901例患者接受了分析(53.5%为大手术):322例使用阿哌沙班,304例使用利伐沙班,267例使用达比加群,8例使用依度沙班。14例(1.6%)患者发生血栓事件,与术前停用DOAC(OR:1.57 [1.03 - 2.4])和无DOAC时间超过6天(OR:5.42 [1.18 - 26])有关。76例(8.4%)患者出现轻微出血事件,达比加群的发生率(12.7%)高于其他DOACs(6.6%)。17例(1.9%)患者发生严重出血事件。315例(35%)患者使用了桥接治疗。它与轻微(OR:2.57 [1.3 - 5.07])和严重(OR:4.2 [1.4 - 12.3])出血事件相关,且未减少血栓事件。本研究提供了关于围手术期DOAC管理及预后的真实世界数据,样本量大且为前瞻性研究,其中大手术比例高。根据药物、出血风险和肾功能进行短期术前DOAC中断,不进行桥接治疗并缩短无DOAC时间,似乎是最安全的做法。