Health Services Management Centre, University of Birmingham, Birmingham, UK.
Int J Health Policy Manag. 2020 Jul 1;9(7):274-285. doi: 10.15171/ijhpm.2019.120.
Childhood vaccination coverage rates in low- and middle-income countries (LMICs) vary significantly, with some countries achieving higher rates than others. Several attempts have been made in Nigeria to achieve universal vaccination coverage but with limited success. This study aimed to analyse strategies used to improve childhood vaccine access and uptake in LMICs in order to inform strategy development for the Nigerian healthcare system.
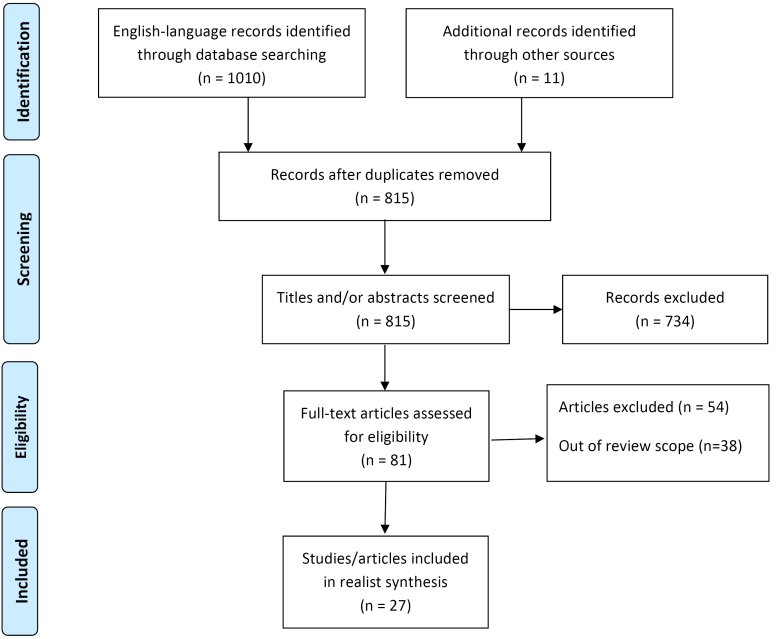
A realist synthesis approach was adopted in order to elucidate the contexts and mechanisms wherewith these strategies achieved their aim (or not). Nine databases were searched for relevant articles and 27 articles were included in the study. Programme theories were generated from the included articles, and data extraction was carried out paying particular attention to context, mechanism and outcomes configurations.
Interventions used in LMICs to improve vaccination coverage were categorised as follows: communication/ educational, reminder-type, incentives, social mobilisation, provider-directed strategies, health service integration and multi-pronged strategies. The strategies that appeared most likely to be effective in the health contexts of contemporary Nigeria include communication and educational interventions; employing informal change agents, and; monitoring and evaluation to strengthen communication. The programme theories for the use of reminders, social mobilisation, staff training and supportive supervision were observed in practice, and these strategies were generally successful within some contexts. By contrast, the use of monetary incentives in Nigeria is not supported by the evidence, although further research and evaluation is required. The integration of other interventions with routine immunisation (RI) to improve uptake was more effective when the perceived value of the other program was high. Adoption of multipronged interventions for hard to reach communities was beneficial. However, caution should be exercised because of varying levels of published evidence in respect of each intervention type and a relative lack of the rich description required to conduct a full realist analysis.
This paper adds to the evidence base on the adaption of strategies to improve vaccine access and uptake to the context of LMICs.
在低收入和中等收入国家(LMICs),儿童疫苗接种覆盖率差异很大,一些国家的覆盖率高于其他国家。尼日利亚曾多次尝试实现普遍疫苗接种覆盖率,但收效甚微。本研究旨在分析旨在改善 LMIC 儿童疫苗获取和接种的策略,以为尼日利亚医疗保健系统的策略制定提供信息。
采用现实主义综合方法,以阐明这些策略实现其目标(或未实现目标)的背景和机制。对九个数据库进行了相关文章搜索,共有 27 篇文章纳入本研究。从纳入的文章中生成了方案理论,并进行了数据提取,特别注意背景、机制和结果配置。
为提高疫苗接种覆盖率而在 LMIC 中使用的干预措施分为以下几类:沟通/教育、提醒型、激励措施、社会动员、提供者导向策略、卫生服务整合和多管齐下的策略。在当代尼日利亚的卫生背景下,似乎最有效的策略包括沟通和教育干预措施;利用非正式的变革推动者;监测和评估以加强沟通。在实践中观察到使用提醒、社会动员、员工培训和支持性监督的方案理论,并且这些策略在某些情况下通常是成功的。相比之下,在尼日利亚,使用金钱激励措施没有得到证据的支持,尽管需要进一步的研究和评估。将其他干预措施与常规免疫(RI)相结合以提高接种率的效果更好,当其他计划的感知价值较高时。采用多管齐下的策略来覆盖难以到达的社区是有益的。然而,应谨慎行事,因为每种干预类型的证据水平不同,并且缺乏进行全面现实主义分析所需的丰富描述。
本文为改善 LMIC 儿童疫苗获取和接种的策略适应背景提供了证据。