Department of Cardiology, Shanghai East Hospital, Tongji University, 1800 Yuntai Rd, Shanghai, 200126, People's Republic of China.
Cardiovascular Medicine of Baoshan People's Hospital of the Yunnan Province, Kunming Medical University, Baoshan, 678000, People's Republic of China.
BMC Cardiovasc Disord. 2020 Jul 11;20(1):330. doi: 10.1186/s12872-020-01604-z.
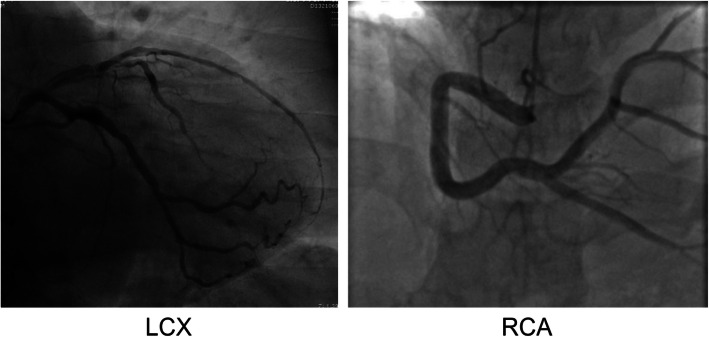
Coronary artery ectasia (CAE) is an angiographic finding of abnormal coronary dilatation. Inflammation plays a major role in all phases of atherosclerosis. We investigated the relationship between CAE and serum high-sensitivity C-reactive protein (hs-CRP) and interleukin-6 (IL-6) levels to test our hypothesis that patient age is associated with the efficacy of anti-inflammatory therapy for CAE.
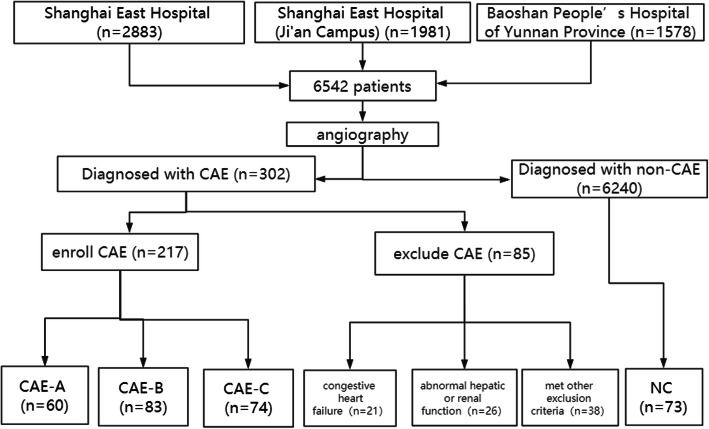
We conducted a prospective analysis of 217 patients with CAE treated at the Department of Cardiology, Shanghai East Hospital, Ji'an Campus and the Baoshan People's Hospital, from January 1, 2015 to July 30, 2019. Baseline data of patients, including sex; age; and history of hypertension, hyperlipidemia, and diabetes, were collected from patient medical records. Study participants were grouped by age as follows: CAE-A (n = 60, age ≤ 50 years), CAE-B (n = 83, 50 years <age ≤ 70 years), and CAE-C (n = 74, age > 70). Additionally, there was a control (NC) group (n = 73) with normal coronary arteries.
All patients received oral rosuvastatin therapy (10 mg, QN quaque nocte) when they were diagnosed with CAE and maintained good follow-up, with a loss rate of 0.0% at the end of the 6-month follow-up. The NC group received regular symptom-relieving treatments and rosuvastatin therapy. Of these four groups, the inflammatory markers, hs-CRP and IL-6, were significantly higher in patients with CAE than in the NCs (p < 0.05). Post-hoc tests showed that hs-CRP and Il-6 levels had significant differences between the CAE-A and CAE-C groups (P = 0.048, P = 0.025). Logistic regression analysis showed that hs-CRP (OR = 1.782, 95% CI: 1.124-2.014, P = 0.021) and IL-6 (OR = 1.584, 95% CI: 1.112-1.986, P = 0.030) were independent predictors of CAE. The inflammatory markers were higher in the CAE-A group than in the CAE-B group and higher in the CAE-B group than in the CAE-C group. Follow-up after 6 months of rosuvastatin therapy showed a significantly greater reduction in hs-CRP and IL-6 levels in the CAE-A group than in the CAE-B group, which again were greater in the CAE-B group than in the CAE-C group.
Anti-inflammatory therapy using rosuvastatin was more effective in younger CAE patients, indicating the need for early statin therapy in CAE.
冠状动脉扩张(CAE)是一种异常冠状动脉扩张的血管造影发现。炎症在动脉粥样硬化的所有阶段都起着重要作用。我们研究了 CAE 与血清高敏 C 反应蛋白(hs-CRP)和白细胞介素-6(IL-6)水平之间的关系,以验证我们的假设,即患者年龄与 CAE 的抗炎治疗效果有关。
我们对 2015 年 1 月 1 日至 2019 年 7 月 30 日期间在上海东方医院吉安校区心内科和宝山区人民医院治疗的 217 例 CAE 患者进行了前瞻性分析。从患者病历中收集患者的基线数据,包括性别、年龄、高血压、高血脂和糖尿病史。根据年龄将研究参与者分为以下三组:CAE-A 组(n=60,年龄≤50 岁)、CAE-B 组(n=83,50 岁<年龄≤70 岁)和 CAE-C 组(n=74,年龄>70 岁)。此外,还有一个正常冠状动脉的对照组(NC 组,n=73)。
所有患者在诊断为 CAE 时均接受口服瑞舒伐他汀治疗(10mg,qn),并进行良好的随访,在 6 个月的随访结束时,失访率为 0.0%。NC 组接受常规对症治疗和瑞舒伐他汀治疗。在这四组中,CAE 患者的炎症标志物 hs-CRP 和 IL-6 明显高于 NC 组(p<0.05)。事后检验显示,CAE-A 组和 CAE-C 组的 hs-CRP 和 Il-6 水平有显著差异(P=0.048,P=0.025)。Logistic 回归分析显示,hs-CRP(OR=1.782,95%CI:1.124-2.014,P=0.021)和 IL-6(OR=1.584,95%CI:1.112-1.986,P=0.030)是 CAE 的独立预测因子。CAE-A 组的炎症标志物高于 CAE-B 组,CAE-B 组高于 CAE-C 组。瑞舒伐他汀治疗 6 个月后的随访显示,CAE-A 组的 hs-CRP 和 IL-6 水平显著低于 CAE-B 组,而 CAE-B 组又显著低于 CAE-C 组。
使用瑞舒伐他汀的抗炎治疗在年轻的 CAE 患者中更有效,这表明 CAE 需要早期进行他汀类药物治疗。