Lancet. 2019 Feb 2;393(10170):407-415. doi: 10.1016/S0140-6736(18)31942-1.
Statin therapy has been shown to reduce major vascular events and vascular mortality in a wide range of individuals, but there is uncertainty about its efficacy and safety among older people. We undertook a meta-analysis of data from all large statin trials to compare the effects of statin therapy at different ages.
In this meta-analysis, randomised trials of statin therapy were eligible if they aimed to recruit at least 1000 participants with a scheduled treatment duration of at least 2 years. We analysed individual participant data from 22 trials (n=134 537) and detailed summary data from one trial (n=12 705) of statin therapy versus control, plus individual participant data from five trials of more intensive versus less intensive statin therapy (n=39 612). We subdivided participants into six age groups (55 years or younger, 56-60 years, 61-65 years, 66-70 years, 71-75 years, and older than 75 years). We estimated effects on major vascular events (ie, major coronary events, strokes, and coronary revascularisations), cause-specific mortality, and cancer incidence as the rate ratio (RR) per 1·0 mmol/L reduction in LDL cholesterol. We compared proportional risk reductions in different age subgroups by use of standard χ tests for heterogeneity when there were two groups, or trend when there were more than two groups.
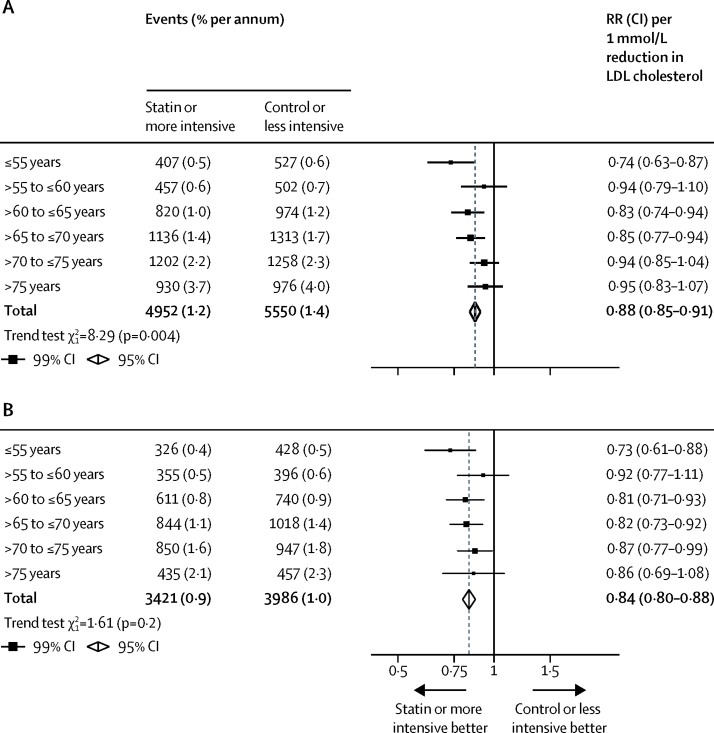
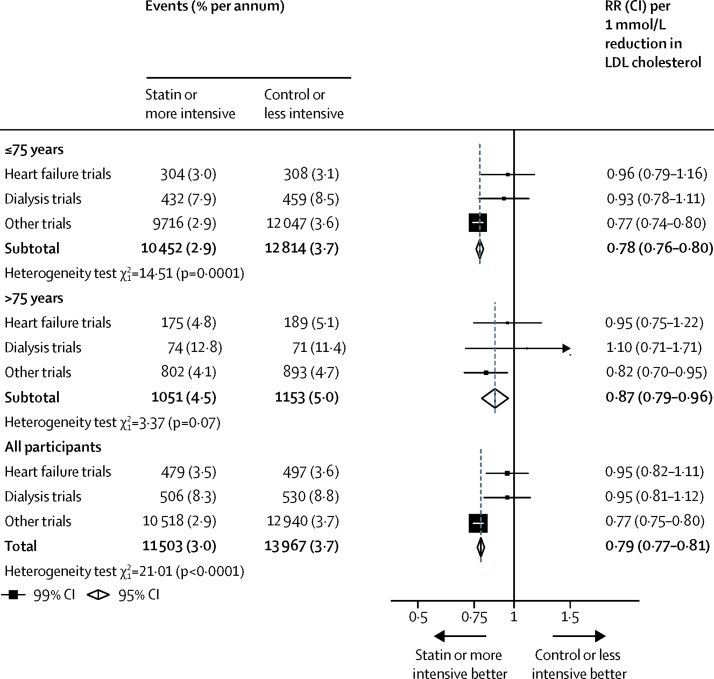
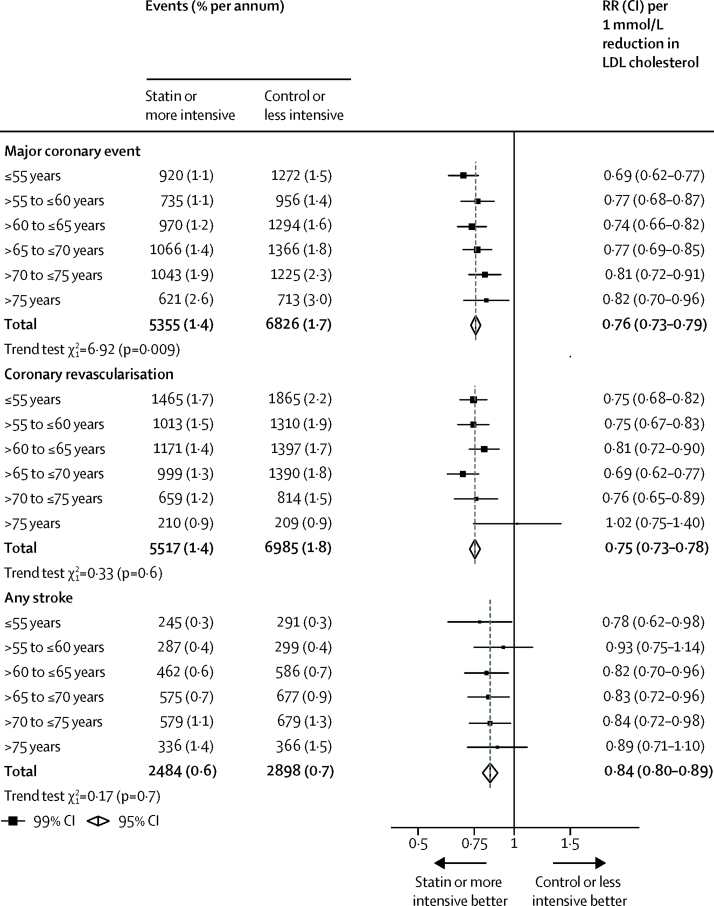
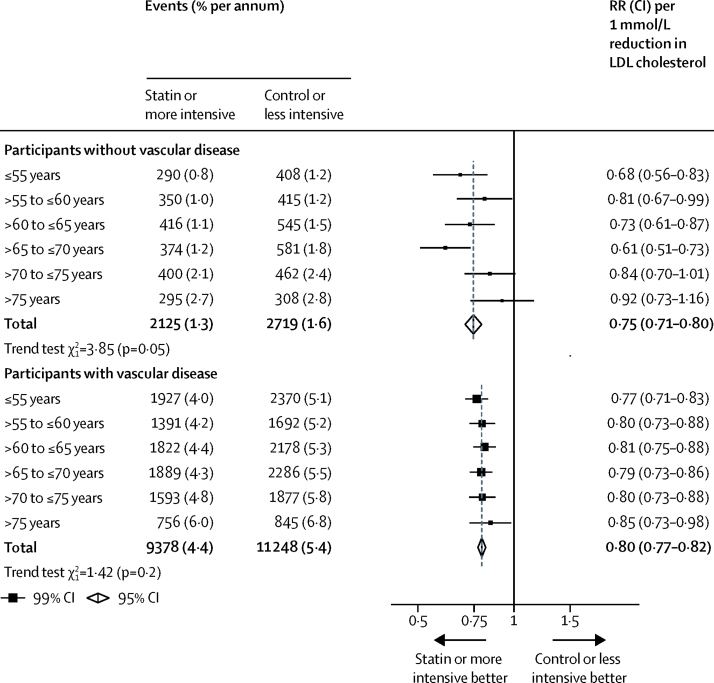
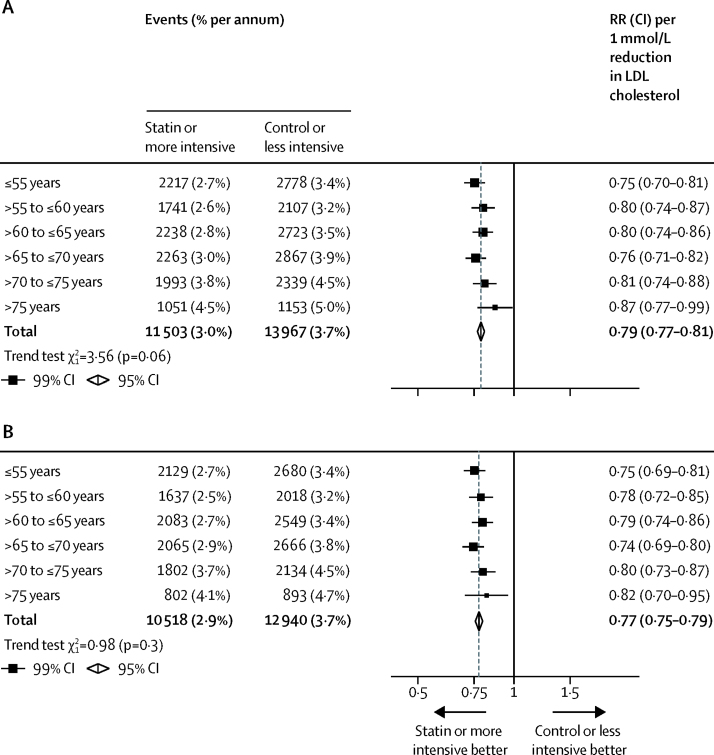
14 483 (8%) of 186 854 participants in the 28 trials were older than 75 years at randomisation, and the median follow-up duration was 4·9 years. Overall, statin therapy or a more intensive statin regimen produced a 21% (RR 0·79, 95% CI 0·77-0·81) proportional reduction in major vascular events per 1·0 mmol/L reduction in LDL cholesterol. We observed a significant reduction in major vascular events in all age groups. Although proportional reductions in major vascular events diminished slightly with age, this trend was not statistically significant (p=0·06). Overall, statin or more intensive therapy yielded a 24% (RR 0·76, 95% CI 0·73-0·79) proportional reduction in major coronary events per 1·0 mmol/L reduction in LDL cholesterol, and with increasing age, we observed a trend towards smaller proportional risk reductions in major coronary events (p=0·009). We observed a 25% (RR 0·75, 95% CI 0·73-0·78) proportional reduction in the risk of coronary revascularisation procedures with statin therapy or a more intensive statin regimen per 1·0 mmol/L lower LDL cholesterol, which did not differ significantly across age groups (p=0·6). Similarly, the proportional reductions in stroke of any type (RR 0·84, 95% CI 0·80-0·89) did not differ significantly across age groups (p=0·7). After exclusion of four trials which enrolled only patients with heart failure or undergoing renal dialysis (among whom statin therapy has not been shown to be effective), the trend to smaller proportional risk reductions with increasing age persisted for major coronary events (p=0·01), and remained non-significant for major vascular events (p=0·3). The proportional reduction in major vascular events was similar, irrespective of age, among patients with pre-existing vascular disease (p=0·2), but appeared smaller among older than among younger individuals not known to have vascular disease (p=0·05). We found a 12% (RR 0·88, 95% CI 0·85-0·91) proportional reduction in vascular mortality per 1·0 mmol/L reduction in LDL cholesterol, with a trend towards smaller proportional reductions with older age (p=0·004), but this trend did not persist after exclusion of the heart failure or dialysis trials (p=0·2). Statin therapy had no effect at any age on non-vascular mortality, cancer death, or cancer incidence.
Statin therapy produces significant reductions in major vascular events irrespective of age, but there is less direct evidence of benefit among patients older than 75 years who do not already have evidence of occlusive vascular disease. This limitation is now being addressed by further trials.
Australian National Health and Medical Research Council, National Institute for Health Research Oxford Biomedical Research Centre, UK Medical Research Council, and British Heart Foundation.
他汀类药物治疗已被证明可降低多种人群的主要血管事件和血管死亡率,但在老年人中,其疗效和安全性仍存在不确定性。我们对所有大型他汀类药物试验的数据进行了荟萃分析,以比较不同年龄组他汀类药物治疗的效果。
在这项荟萃分析中,只要他汀类药物治疗的预定治疗持续时间至少为 2 年,且试验旨在招募至少 1000 名参与者,即可纳入随机试验。我们分析了来自 22 项试验(n=134537 名参与者)的个体参与者数据和来自 1 项试验(n=12705 名参与者)的详细汇总数据,该试验比较了他汀类药物治疗与对照组的效果,以及来自 5 项比较更强化与更弱化他汀类药物治疗的试验(n=39612 名参与者)的个体参与者数据。我们将参与者分为 6 个年龄组(55 岁或以下、56-60 岁、61-65 岁、66-70 岁、71-75 岁和 75 岁以上)。我们估计了主要血管事件(即主要冠状动脉事件、中风和冠状动脉血运重建)、特定原因死亡率和癌症发病率的影响,其效应值为 LDL 胆固醇每降低 1.0mmol/L 的率比(RR)。我们使用标准 χ2 检验比较不同年龄亚组的比例风险降低,如果有两组,则进行异质性检验,如果有多于两组,则进行趋势检验。
在 28 项试验中,186854 名参与者中有 14483 名(8%)在随机分组时年龄大于 75 岁,中位随访时间为 4.9 年。总体而言,他汀类药物治疗或更强化的他汀类药物治疗方案可使 LDL 胆固醇每降低 1.0mmol/L,主要血管事件的比例风险降低 21%(RR 0.79,95%CI 0.77-0.81)。我们观察到所有年龄组的主要血管事件都有显著减少。尽管主要血管事件的比例风险降低随着年龄的增长而略有减少,但这种趋势无统计学意义(p=0.06)。总体而言,他汀类药物或更强化治疗可使 LDL 胆固醇每降低 1.0mmol/L,主要冠状动脉事件的比例风险降低 24%(RR 0.76,95%CI 0.73-0.79),并且随着年龄的增长,我们观察到主要冠状动脉事件的比例风险降低幅度有变小的趋势(p=0.009)。我们观察到,他汀类药物治疗或更强化治疗方案可使 LDL 胆固醇每降低 1.0mmol/L,冠状动脉血运重建手术的风险降低 25%(RR 0.75,95%CI 0.73-0.78),这种风险降低在不同年龄组之间没有显著差异(p=0.6)。同样,任何类型中风的比例风险降低(RR 0.84,95%CI 0.80-0.89)在不同年龄组之间也没有显著差异(p=0.7)。排除了 4 项仅纳入心力衰竭或接受肾脏透析患者的试验(在这些患者中,他汀类药物治疗尚未被证明有效)后,主要冠状动脉事件的比例风险降低幅度随年龄增长而减小的趋势仍然存在(p=0.01),但对于主要血管事件,这种趋势仍不显著(p=0.3)。在有或没有先前存在的血管疾病的患者中,主要血管事件的比例风险降低幅度相似(p=0.2),但在年龄较大的患者中似乎较小,而在没有血管疾病的年龄较小的患者中则没有这种情况(p=0.05)。我们发现,LDL 胆固醇每降低 1.0mmol/L,血管死亡率降低 12%(RR 0.88,95%CI 0.85-0.91),随着年龄的增长,这种比例风险降低有变小的趋势(p=0.004),但这种趋势在排除心力衰竭或透析试验后并不存在(p=0.2)。他汀类药物治疗在任何年龄对非血管性死亡率、癌症死亡或癌症发病率均无影响。
他汀类药物治疗可显著降低主要血管事件的发生风险,无论年龄大小,但在没有证据表明存在闭塞性血管疾病的 75 岁以上患者中,其直接获益证据较少。目前正在通过进一步的试验来解决这一局限性。
澳大利亚国家卫生和医学研究委员会、英国国家卫生研究院牛津生物医学研究中心、英国医学研究理事会和英国心脏基金会。