Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia; Department of Gynecology and Obstetrics, School of Medicine, Emory University, Atlanta, Georgia.
Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia.
Fertil Steril. 2020 Sep;114(3):567-578. doi: 10.1016/j.fertnstert.2020.04.004. Epub 2020 Jul 14.
To assess trends, predictors, and perinatal outcomes of ovarian hyperstimulation syndrome (OHSS) associated with in vitro fertilization (IVF) cycles in the United States.
Retrospective cohort study using National Assisted Reproductive Technology Surveillance System (NASS) data.
Not applicable.
PATIENT(S): Fresh autologous and embryo-banking cycles performed from 2000 to 2015.
INTERVENTIONS(S): None.
MAIN OUTCOME MEASURE(S): OHSS, first-trimester loss, second-trimester loss, stillbirth, low birth weight, and preterm delivery.
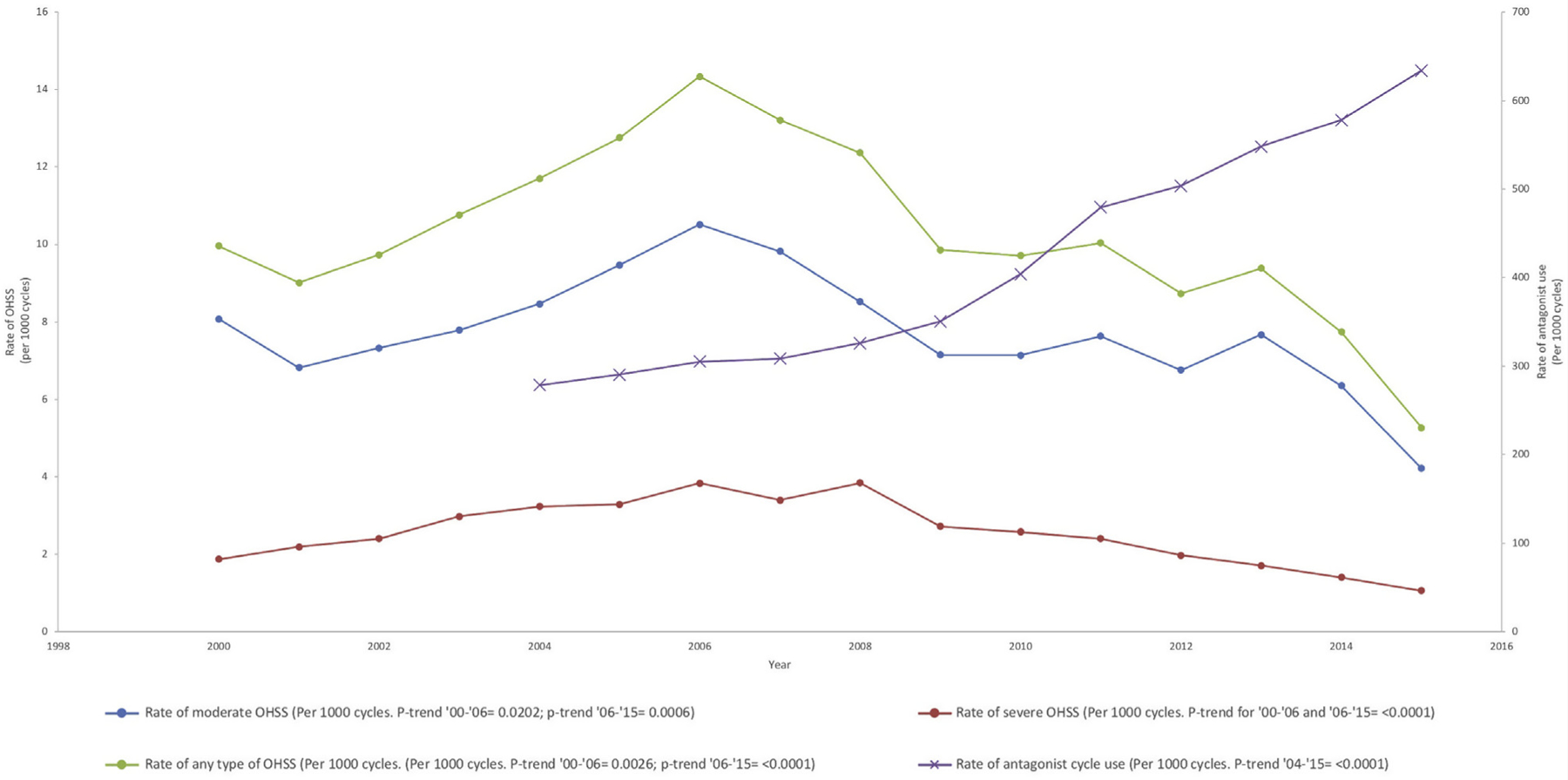
RESULT(S): The proportion of IVF cycles complicated by OHSS increased from 10.0 to 14.3 cases per 1,000 from 2000 to 2006, and decreased to 5.3 per 1,000 from 2006 to 2015. The risk of OHSS was highest for cycles with more than 30 oocytes retrieved (adjusted risk ratio [aRR] 3.85). OHSS was associated with a diagnosis of ovulatory disorder (aRR 2.61), tubal factor (aRR 1.14), uterine factor (aRR 1.17) and cycles resulting in pregnancy (aRR 3.12). In singleton pregnancies, OHSS was associated with increased risk of low birth weight (aRR 1.29) and preterm delivery (aRR 1.32). In twin pregnancies, OHSS was associated with an increased risk of second-trimester loss (aRR 1.81), low birth weight (aRR 1.06), and preterm delivery (aRR 1.16).
CONCLUSION(S): Modifiable predictive factors for OHSS include number of oocytes retrieved, pregnancy following fresh embryo transfer, and the type of medication used for pituitary suppression during controlled ovarian hyperstimulation. Patients affected by OHSS had a higher risk of preterm delivery and low birth weight. Clinicians should take measures to reduce the risk of OHSS whenever possible.
评估美国体外受精(IVF)周期中与卵巢过度刺激综合征(OHSS)相关的趋势、预测因素和围产期结局。
使用国家辅助生殖技术监测系统(NASS)数据的回顾性队列研究。
不适用。
2000 年至 2015 年进行的新鲜自体和胚胎冷冻周期。
无。
OHSS、孕早期流产、孕中期流产、死产、低出生体重和早产。
2000 年至 2006 年,每 1000 个 IVF 周期中由 OHSS 引起的比例从 10.0 例增加到 14.3 例,而 2006 年至 2015 年则降至 5.3 例。取卵超过 30 个的周期发生 OHSS 的风险最高(调整后的风险比[aRR]3.85)。OHSS 与排卵障碍(aRR 2.61)、输卵管因素(aRR 1.14)、子宫因素(aRR 1.17)和导致妊娠的周期(aRR 3.12)有关。在单胎妊娠中,OHSS 与低出生体重(aRR 1.29)和早产(aRR 1.32)的风险增加有关。在双胎妊娠中,OHSS 与孕中期流产(aRR 1.81)、低出生体重(aRR 1.06)和早产(aRR 1.16)的风险增加有关。
OHSS 的可修改预测因素包括取卵数、新鲜胚胎移植后妊娠以及控制性卵巢过度刺激期间用于抑制垂体的药物类型。患有 OHSS 的患者早产和低出生体重的风险较高。临床医生应尽可能采取措施降低 OHSS 的风险。