Martin Shedrick, Tallian Kimberly, Nguyen Victoria T, van Dyke Jason, Sikand Harminder
Clinical Pharmacist Specialist, Santa Rosa Memorial Hospital, Santa Rosa, California.
Clinical Pharmacist, Providence Little Company of Mary Medical Center, San Pedro, California.
Ment Health Clin. 2020 Jul 2;10(4):215-221. doi: 10.9740/mhc.2020.07.215. eCollection 2020 Jul.
Chronic lower back pain is a leading cause of disability in US adults. Opioid use continues to be controversial despite the Centers for Disease Control and Prevention guidance on chronic pain management to use nonpharmacologic and nonopioid pharmacologic interventions. The objectives of the study were to assess the impact of early physical therapy (PT) intervention on improving functionality and reducing opioid burden in patients with chronic lower back pain.
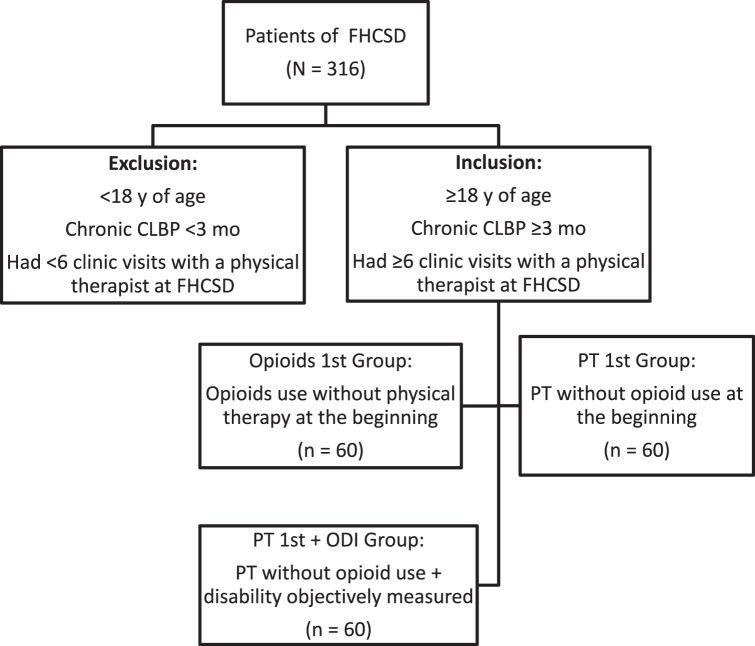
A single-center, retrospective chart review of patients receiving ≥6 PT visits and treated with either opioids first (OF) or PT first (PTF) therapy for chronic lower back pain were evaluated. Concomitant use of nonopioid and nonpharmacologic therapy was permitted. The Oswestry Disability Index (ODI), a survey measuring functionality, was recorded for PTF group. Pain scores and medication use including opioids were collected at treatment initiation and completion.
One hundred and eighty patients were included in three groups: OF group (n = 60), PTF group (n = 60), and PTF + ODI group (n = 60). The PTF + ODI group had mean ODI reduction of 11.9% ( < .001). More OF patients were lost to follow up (68.3%) or failed PT (60%) compared to the PTF group, 38.3% and 3.3% ( < .001). Reduction in both opioid and nonopioid medications as well as pain scores were observed but not statistically significant.
Early PT resulted in improved functionality, decreased pain, and reduced medication use upon PT completion. These findings suggest PT, along with nonopioid modalities, are a viable first-line option for the management of chronic lower back pain.
慢性下腰痛是美国成年人残疾的主要原因。尽管疾病控制与预防中心针对慢性疼痛管理给出了使用非药物和非阿片类药物干预措施的指导意见,但阿片类药物的使用仍然存在争议。本研究的目的是评估早期物理治疗(PT)干预对改善慢性下腰痛患者功能和减轻阿片类药物负担的影响。
对接受≥6次PT治疗且因慢性下腰痛接受阿片类药物优先治疗(OF)或PT优先治疗(PTF)的患者进行单中心回顾性病历审查。允许同时使用非阿片类药物和非药物治疗。记录PTF组用于测量功能的Oswestry残疾指数(ODI)。在治疗开始和结束时收集疼痛评分和包括阿片类药物在内的药物使用情况。
180名患者被纳入三组:OF组(n = 60)、PTF组(n = 60)和PTF + ODI组(n = 60)。PTF + ODI组的ODI平均降低了11.9%(P < .001)。与PTF组相比,更多接受OF治疗的患者失访(68.3%)或PT治疗失败(60%),PTF组分别为38.3%和3.3%(P < .001)。观察到阿片类药物和非阿片类药物的使用以及疼痛评分均有所降低,但差异无统计学意义。
早期PT在PT治疗结束后可改善功能、减轻疼痛并减少药物使用。这些发现表明,PT与非阿片类治疗方法一起,是管理慢性下腰痛的可行一线选择。