Wheeler Kathleen E, Grilli Ryan, Centofanti John E, Martin Janet, Gelinas Celine, Szumita Paul M, Devlin John W, Chanques Gerald, Alhazzani Waleed, Skrobik Yoanna, Kho Michelle E, Nunnally Mark E, Gagarine Andre, Ergan Begum A, Fernando Shannon, Price Carrie, Lewin John, Rochwerg Bram
Department of Anesthesia, McMaster University, Hamilton, ON, Canada.
Division of Critical Care, McMaster University, Hamilton, ON, Canada.
Crit Care Explor. 2020 Jul 6;2(7):e0157. doi: 10.1097/CCE.0000000000000157. eCollection 2020 Jul.
This systematic review and meta-analysis addresses the efficacy and safety of nonopioid adjunctive analgesics for patients in the ICU.
We searched PubMed, Embase, the Cochrane Library, CINAHL Plus, and Web of Science.
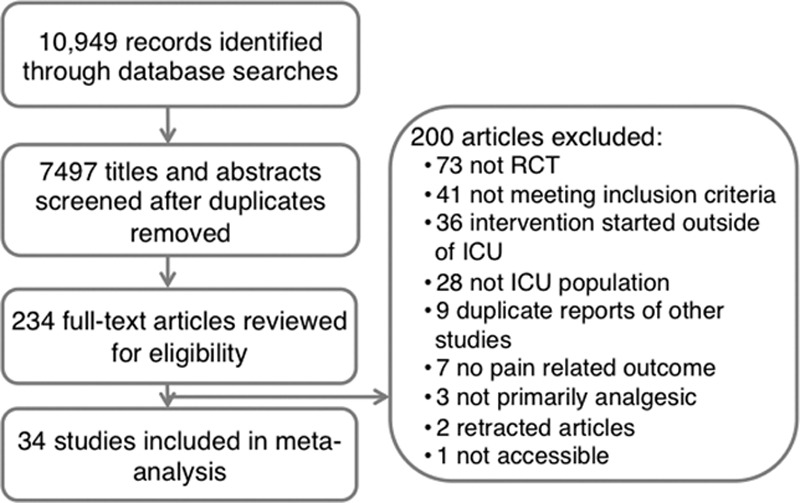
Two independent reviewers screened citations. Eligible studies included randomized controlled trials comparing efficacy and safety of an adjuvant-plus-opioid regimen to opioids alone in adult ICU patients.
We conducted duplicate screening of citations and data abstraction.
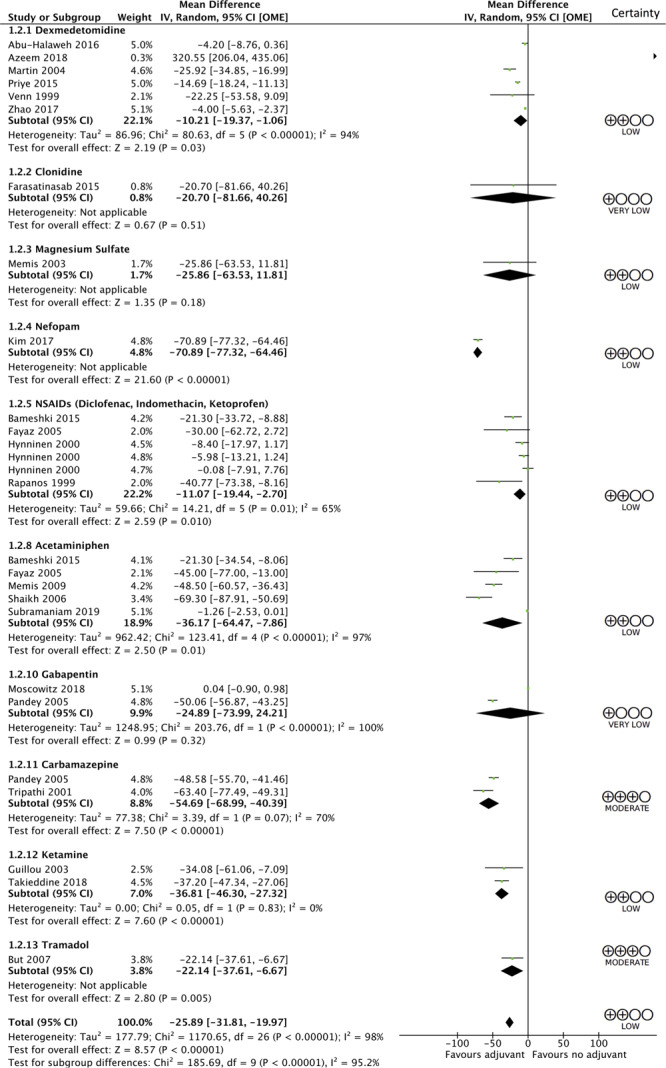
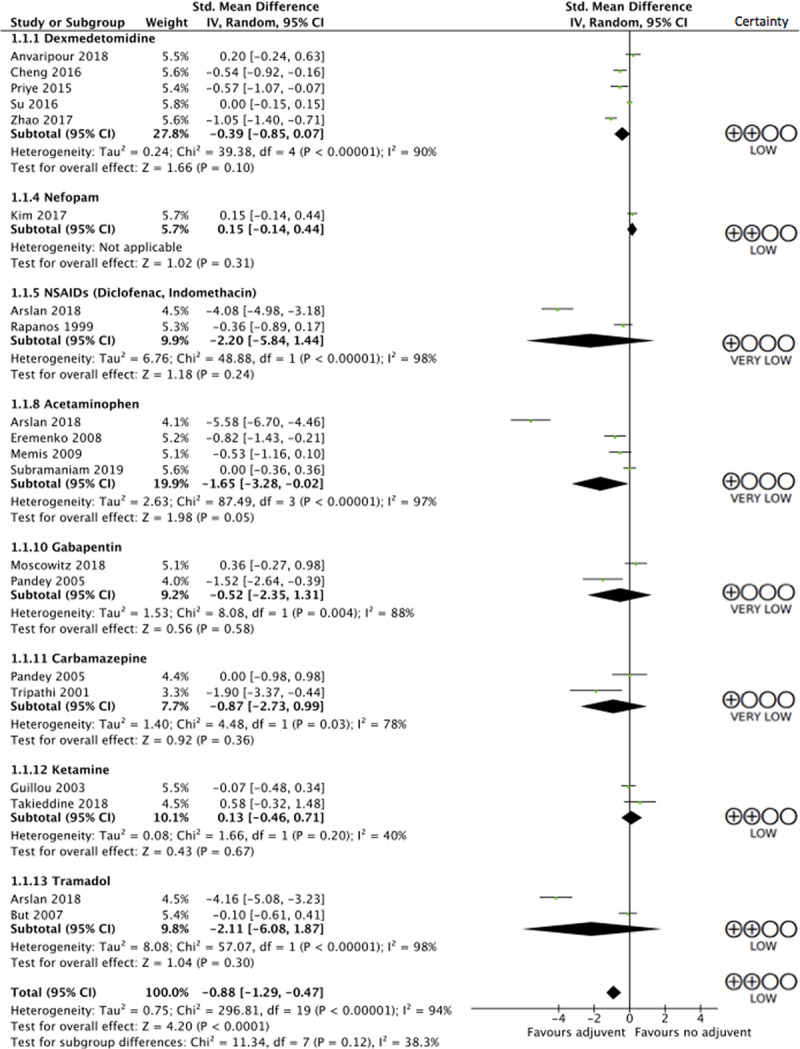
Of 10,949 initial citations, we identified 34 eligible trials. These trials examined acetaminophen, carbamazepine, clonidine, dexmedetomidine, gabapentin, ketamine, magnesium sulfate, nefopam, nonsteroidal anti-inflammatory drugs (including diclofenac, indomethacin, and ketoprofen), pregabalin, and tramadol as adjunctive analgesics. Use of any adjuvant in addition to an opioid as compared to an opioid alone led to reductions in patient-reported pain scores at 24 hours (standard mean difference, -0.88; 95% CI, -1.29 to -0.47; low certainty) and decreased opioid consumption (in oral morphine equivalents over 24 hr; mean difference, 25.89 mg less; 95% CI, 19.97-31.81 mg less; low certainty). In terms of individual medications, reductions in opioid use were demonstrated with acetaminophen (mean difference, 36.17 mg less; 95% CI, 7.86-64.47 mg less; low certainty), carbamazepine (mean difference, 54.69 mg less; 95% CI, 40.39-to 68.99 mg less; moderate certainty), dexmedetomidine (mean difference, 10.21 mg less; 95% CI, 1.06-19.37 mg less; low certainty), ketamine (mean difference, 36.81 mg less; 95% CI, 27.32-46.30 mg less; low certainty), nefopam (mean difference, 70.89 mg less; 95% CI, 64.46-77.32 mg less; low certainty), nonsteroidal anti-inflammatory drugs (mean difference, 11.07 mg less; 95% CI, 2.7-19.44 mg less; low certainty), and tramadol (mean difference, 22.14 mg less; 95% CI, 6.67-37.61 mg less; moderate certainty).
Clinicians should consider using adjunct agents to limit opioid exposure and improve pain scores in critically ill patients.
本系统评价和荟萃分析探讨了非阿片类辅助镇痛药对重症监护病房(ICU)患者的疗效和安全性。
我们检索了PubMed、Embase、Cochrane图书馆、CINAHL Plus和Web of Science。
两名独立评审员筛选文献。符合条件的研究包括随机对照试验,比较辅助药物加阿片类药物方案与单纯阿片类药物在成年ICU患者中的疗效和安全性。
我们对文献和数据进行了重复筛选和提取。
在10949篇初始文献中,我们确定了34项符合条件的试验。这些试验研究了对乙酰氨基酚、卡马西平、可乐定、右美托咪定、加巴喷丁、氯胺酮、硫酸镁、奈福泮、非甾体抗炎药(包括双氯芬酸、吲哚美辛和酮洛芬)、普瑞巴林和曲马多作为辅助镇痛药的情况。与单纯使用阿片类药物相比,联合使用任何一种辅助药物可使患者报告的24小时疼痛评分降低(标准平均差,-0.88;95%置信区间,-1.29至-0.47;低确定性),并减少阿片类药物的消耗量(以24小时口服吗啡当量计;平均差,少25.89mg;95%置信区间,少19.97 - 31.81mg;低确定性)。就个别药物而言,对乙酰氨基酚(平均差,少36.17mg;95%置信区间,少7.86 - 64.47mg;低确定性)、卡马西平(平均差,少54.69mg;95%置信区间,少40.39至68.99mg;中等确定性)、右美托咪定(平均差,少10.21mg;95%置信区间,少1.06 - 19.37mg;低确定性)、氯胺酮(平均差,少36.81mg;95%置信区间,少27.32 - 46.30mg;低确定性)、奈福泮(平均差,少70.89mg;95%置信区间,少64.46 - 77.32mg;低确定性)、非甾体抗炎药(平均差,少11.07mg;95%置信区间,少2.7 - 19.44mg;低确定性)和曲马多(平均差,少22.14mg;95%置信区间,少6.67 - 37.61mg;中等确定性)均显示可减少阿片类药物的使用。
临床医生应考虑使用辅助药物来减少重症患者的阿片类药物暴露并改善疼痛评分。