Department of Family and Community Medicine, University of Toronto, Toronto, Ontario, Canada.
Bridgepoint Collaboratory for Research and Innovation, Lunenfeld-Tanenbaum Research Institute, Sinai Health System, Toronto, Ontario, Canada.
PLoS One. 2020 Jul 27;15(7):e0236419. doi: 10.1371/journal.pone.0236419. eCollection 2020.
Opioid related deaths are at epidemic levels in many developed nations globally. Concerns about the contribution of prescribed opioids, and particularly high-dose opioids, continue to mount as do initiatives to reduce prescribing. Evidence around opioid tapering, which can be challenging and potentially hazardous, is not well developed. A recent national guideline has recognized this and recommended referral to multidisciplinary care for challenging cases of opioid tapering. However, multidisciplinary care for opioid tapering is not well understood or defined.
Identify the existing literature on any multidisciplinary care programs that evaluate impact on opioid use, synthesize how these programs work and clarify whom they benefit.
Systematic rapid realist review.
Bibliographic databases (MEDLINE, EMBASE, CINAHL, PsycINFO, Cochrane Library), grey literature, reference hand search and formal expert consultation.
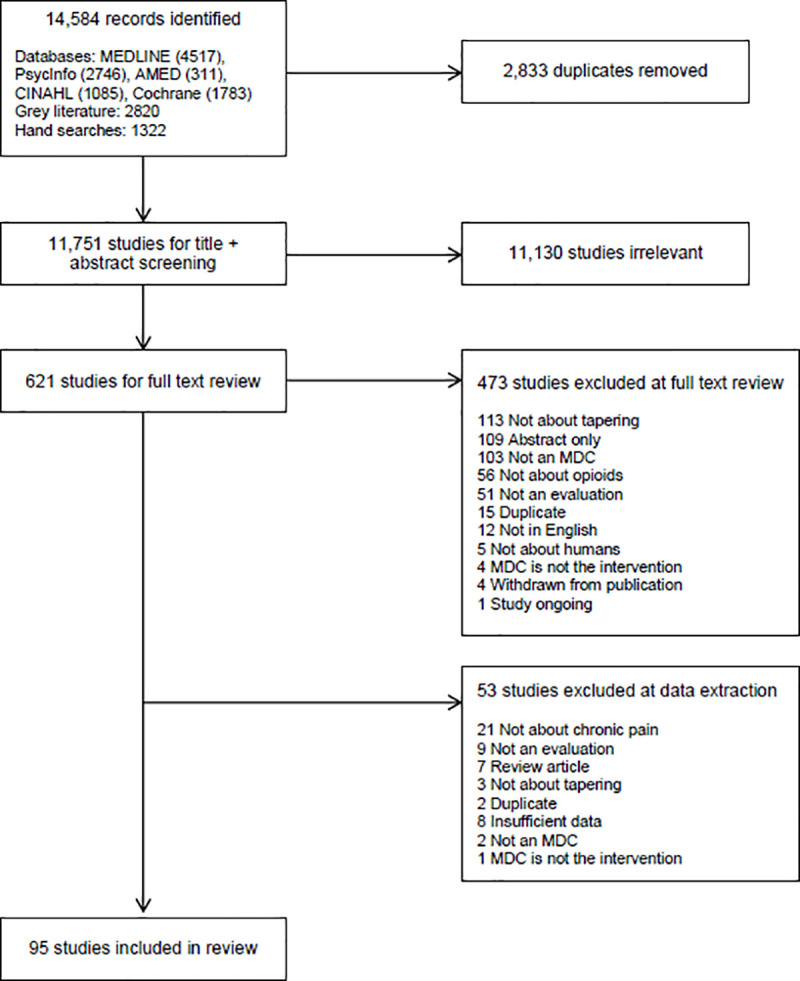
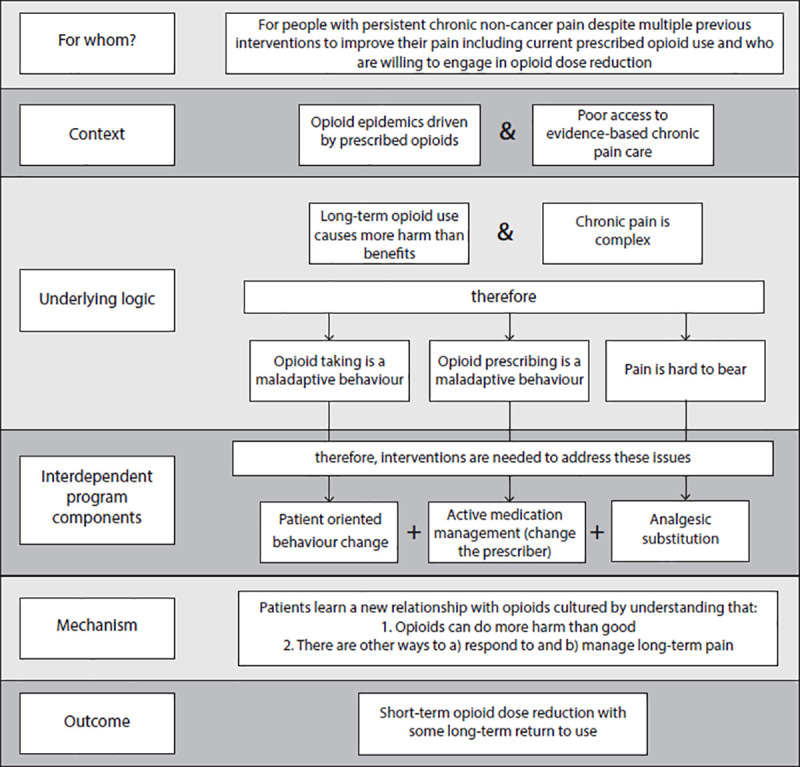
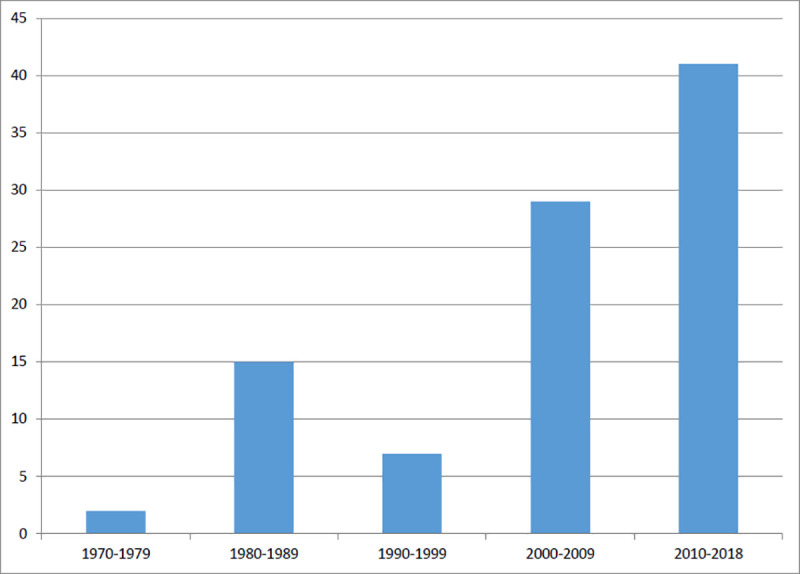
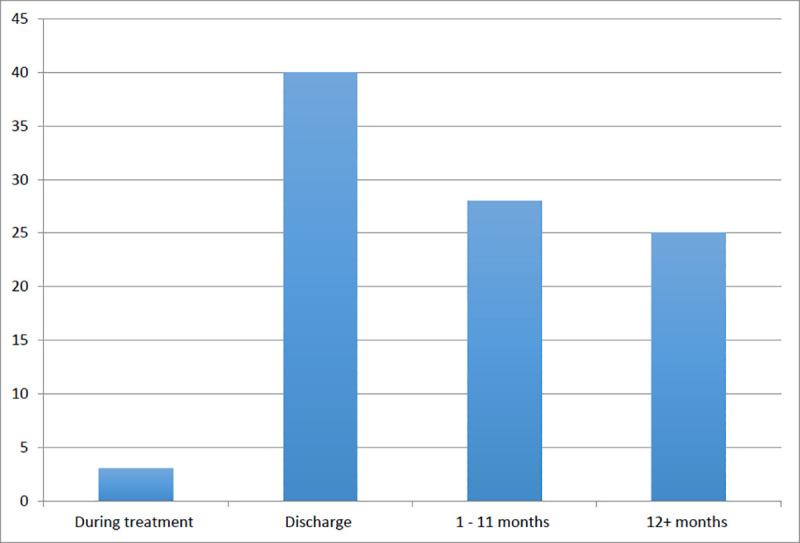
95 studies were identified. 75% of the programs were from the United States and the majority (n = 62) were published after 2000. A minority (n = 23) of programs reported on >12 month opioid use outcomes. There were three necessary but insufficient mechanisms common to all programs: pain relief, behavior change and active medication management. Programs that did not include a combination of all three mechanisms did not result in opioid dose reductions. A concerning 20-40% of subjects resumed opioid use within one year of program completion.
Providing alternative analgesia is insufficient for reducing opioid doses. Even high quality primary care multidisciplinary care programs do not reduce prescribed opioid use unless there is active medication management accomplished by changing the primary opioid prescriber. Rates of return to use of opioids from these programs are very concerning in the current context of a highly potent and lethal street drug supply. This contextual factor may be powerful enough to undermine the modest benefits of opioid dose reduction via multidisciplinary care.
在许多发达国家,阿片类药物相关死亡人数处于流行水平。随着减少处方的举措不断增加,人们对处方阿片类药物(尤其是高剂量阿片类药物)的作用的担忧也与日俱增。阿片类药物逐渐减量的证据尚不完善,且可能具有挑战性和潜在危险。最近的一项国家指南已经认识到这一点,并建议将有挑战性的阿片类药物逐渐减量病例转介给多学科护理。然而,多学科护理阿片类药物逐渐减量的理解和定义还不够完善。
确定评估阿片类药物使用影响的任何多学科护理计划的现有文献,综合这些计划的工作方式,并阐明它们对谁有益。
系统快速真实主义审查。
文献数据库(MEDLINE、EMBASE、CINAHL、PsycINFO、Cochrane 图书馆)、灰色文献、参考文献手工搜索和正式专家咨询。
共确定了 95 项研究。75%的计划来自美国,其中大多数(n=62)发表于 2000 年后。少数(n=23)计划报告了>12 个月的阿片类药物使用结果。所有计划都有三个必要但不充分的机制:缓解疼痛、行为改变和积极的药物管理。没有结合所有三个机制的计划不会导致阿片类药物剂量减少。令人担忧的是,20-40%的受试者在计划完成后一年内重新开始使用阿片类药物。
提供替代镇痛不足以减少阿片类药物剂量。即使是高质量的初级保健多学科护理计划,如果没有通过改变主要阿片类药物开方者来实现积极的药物管理,也不能减少处方阿片类药物的使用。在当前高度有效和致命的街头毒品供应背景下,这些计划中重新使用阿片类药物的比例非常令人担忧。这种背景因素可能足以削弱通过多学科护理减少阿片类药物剂量的适度益处。