Independent Statistical Analyst, Seattle, Washington.
Exergen Corporation, Watertown, Massachusetts.
West J Emerg Med. 2020 Jun 24;21(4):909-917. doi: 10.5811/westjem.2020.3.45215.
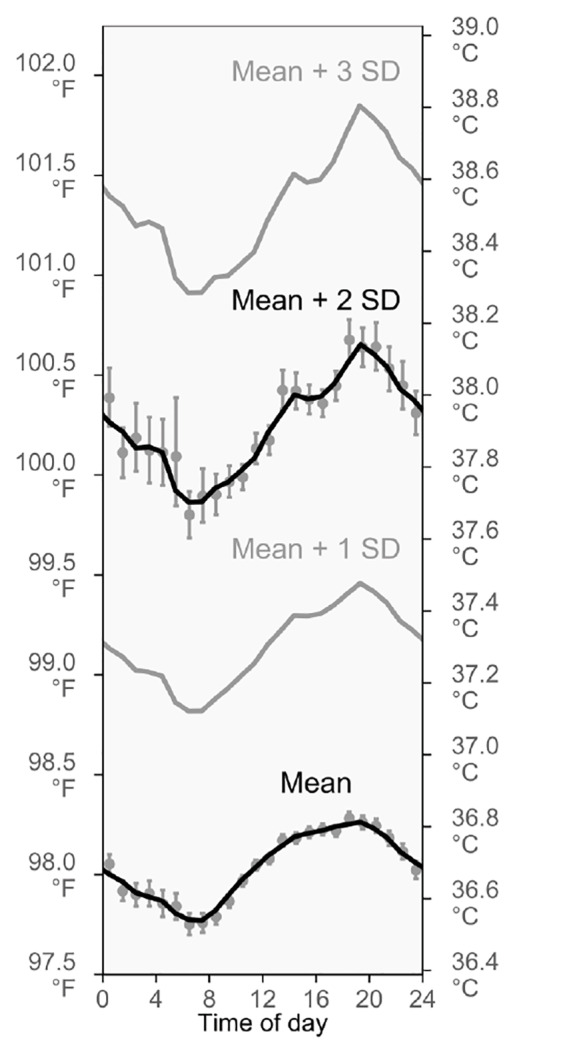
In this observational study, we evaluated time-of-day variation in the incidence of fever that is seen at triage. The observed incidence of fever could change greatly over the day because body temperatures generally rise and fall in a daily cycle, yet fever is identified using a temperature threshold that is unchanging, such as ≥38.0° Celsius (C) (≥100.4° Fahrenheit [F]).
We analyzed 93,225 triage temperature measurements from a Boston emergency department (ED) (2009-2012) and 264,617 triage temperature measurements from the National Hospital Ambulatory Medical Care Survey (NHAMCS, 2002-2010), making this the largest study of body temperature since the mid-1800s. Boston data were investigated exploratorily, while NHAMCS was used to corroborate Boston findings and check whether they generalized. NHAMCS results are nationally representative of United States EDs. Analyses focused on adults.
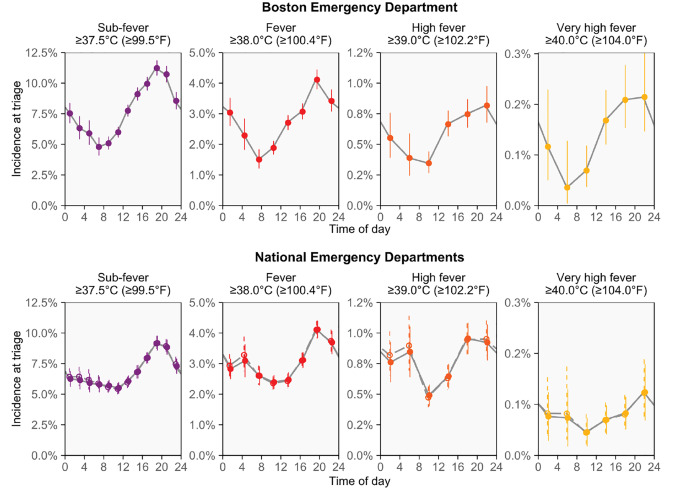
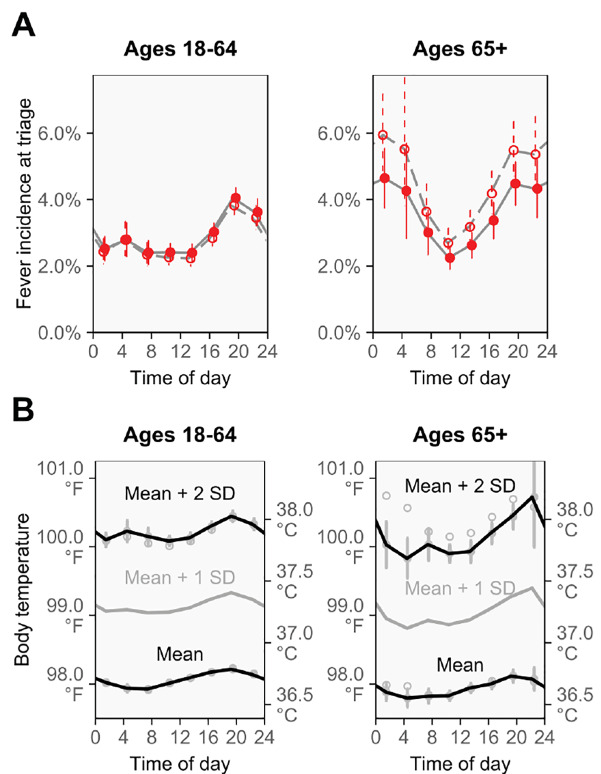
In the Boston ED, the proportion of patients with triage temperatures in the fever range (≥38.0°C, ≥100.4°F) increased 2.5-fold from morning to evening (7:00-8:59 PM vs 7:00-8:59 AM: risk ratio [RR] 2.5, 95% confidence interval [CI], 2.0-3.3). Similar time-of-day changes were observed when investigating alternative definitions of fever: temperatures ≥39.0°C (≥102.2°F) and ≥40.0°C (≥104.0°F) increased 2.4- and 3.6-fold from morning to evening (7:00-8:59 PM vs 7:00-8:59 AM: RRs [95% CIs] 2.4 [1.5-4.3] and 3.6 [1.5-17.7], respectively). Analyses of adult NHAMCS patients provided confirmation, showing mostly similar increases for the same fever definitions and times of day (RRs [95% CIs] 1.8 [1.6-2.1], 1.9 [1.4-2.5], and 2.8 [0.8-9.3], respectively), including after adjusting for 12 potential confounders using multivariable regression (adjusted RRs [95% CIs] 1.8 [1.5-2.1], 1.8 [1.3-2.4], and 2.7 [0.8-9.2], respectively), in age-group analyses (18-64 vs 65+ years), and in several sensitivity analyses. The patterns observed for fever mirror the circadian rhythm of body temperature, which reaches its highest and lowest points at similar times.
Fever incidence is lower at morning triages than at evening triages. High fevers are especially rare at morning triage and may warrant special consideration for this reason. Studies should examine whether fever-causing diseases are missed or underappreciated during mornings, especially for sepsis cases and during screenings for infectious disease outbreaks. The daily cycling of fever incidence may result from the circadian rhythm.
在这项观察性研究中,我们评估了分诊时发热的时间变化。由于体温通常呈昼夜节律变化,因此观察到的发热发生率可能会有很大变化,但发热是通过使用不变的温度阈值(例如≥38.0°C(≥100.4°F))来识别的。
我们分析了来自波士顿急诊部(ED)的 93225 次分诊体温测量值(2009-2012 年)和来自全国医院门诊医疗保健调查(NHAMCS,2002-2010 年)的 264617 次分诊体温测量值,这是自 19 世纪中叶以来对体温进行的最大研究。对波士顿数据进行了探索性分析,而 NHAMCS 则用于证实波士顿的发现并检查它们是否具有普遍性。NHAMCS 的结果代表了美国 ED 的全国情况。分析主要集中在成年人身上。
在波士顿 ED,从早上到晚上(下午 7:00-8:59 与上午 7:00-8:59),发热(≥38.0°C,≥100.4°F)患者的比例增加了 2.5 倍(风险比[RR] 2.5,95%置信区间[CI],2.0-3.3)。当研究替代发热定义时,观察到类似的昼夜变化:体温≥39.0°C(≥102.2°F)和≥40.0°C(≥104.0°F)的比例分别从早上到晚上增加了 2.4-和 3.6 倍(下午 7:00-8:59 与上午 7:00-8:59:RR [95% CIs] 2.4 [1.5-4.3] 和 3.6 [1.5-17.7])。对成人 NHAMCS 患者的分析提供了证实,显示相同的发热定义和时间出现了相似的增加(RRs [95% CIs] 1.8 [1.6-2.1]、1.9 [1.4-2.5]和 2.8 [0.8-9.3]),包括在使用多变量回归调整 12 个潜在混杂因素后(调整后的 RRs [95% CIs] 1.8 [1.5-2.1]、1.8 [1.3-2.4]和 2.7 [0.8-9.2]),在年龄组分析(18-64 岁与 65 岁以上)和几项敏感性分析中。发热的发生模式反映了体温的昼夜节律,体温在相似的时间达到最高和最低点。
早晨的分诊比晚上的分诊发热发生率低。上午的分诊中,高热特别罕见,因此可能需要特别注意。研究应检查在早晨是否会错过或低估发热性疾病,尤其是在脓毒症病例和传染病爆发筛查期间。发热发生率的每日循环可能是由于昼夜节律引起的。