Department of Microbiology, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
Student Research Committee, Iran University of Medical Sciences, Tehran, Iran.
Sci Rep. 2020 Jul 29;10(1):12689. doi: 10.1038/s41598-020-69058-z.
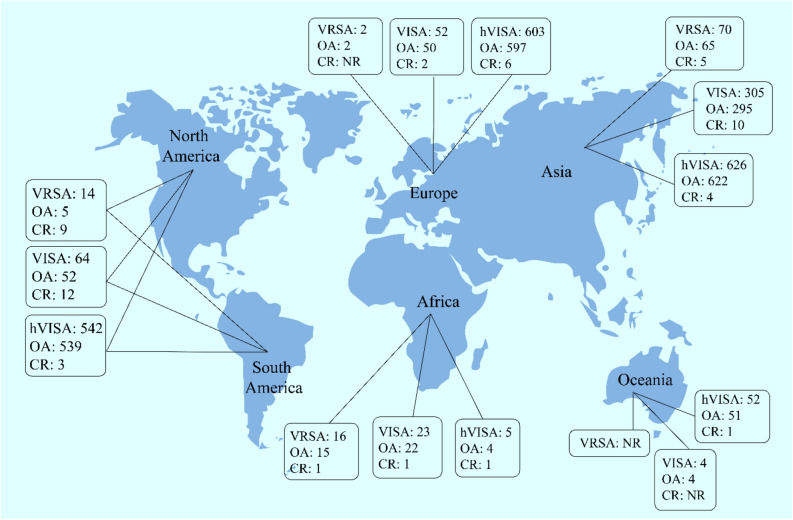
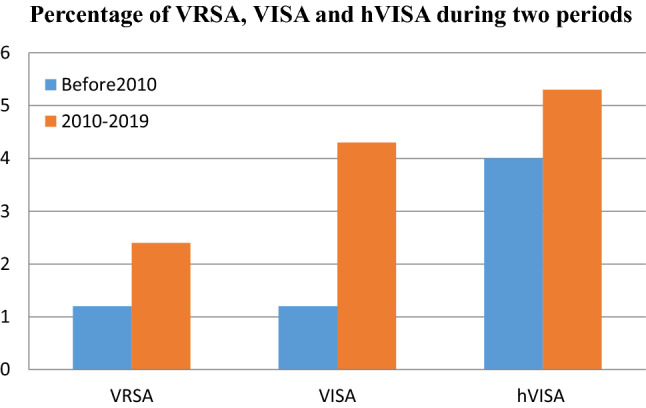
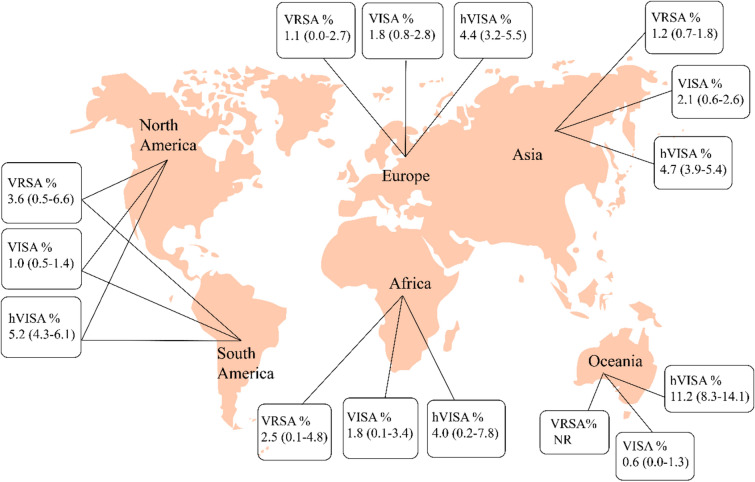
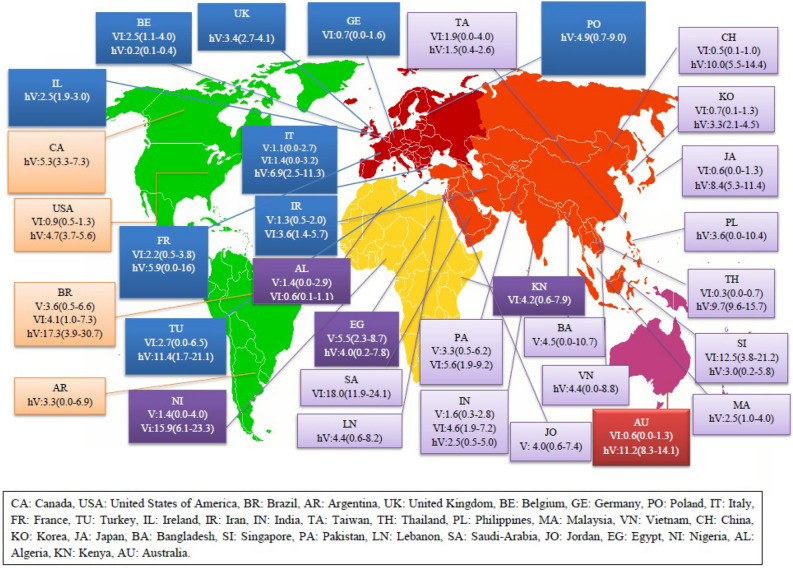
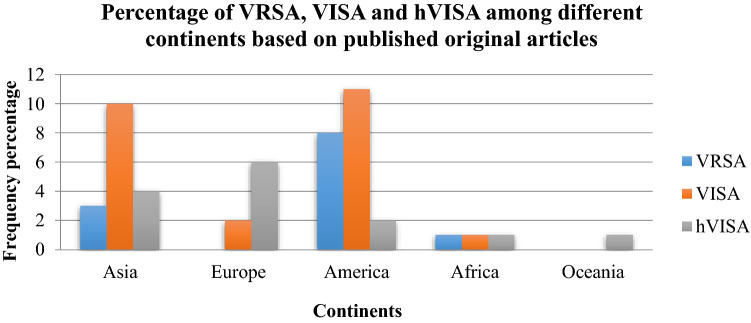
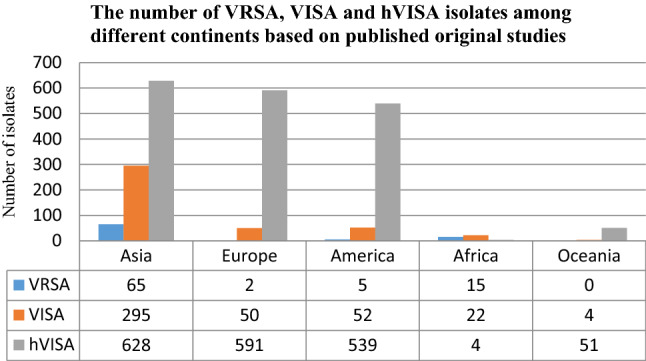
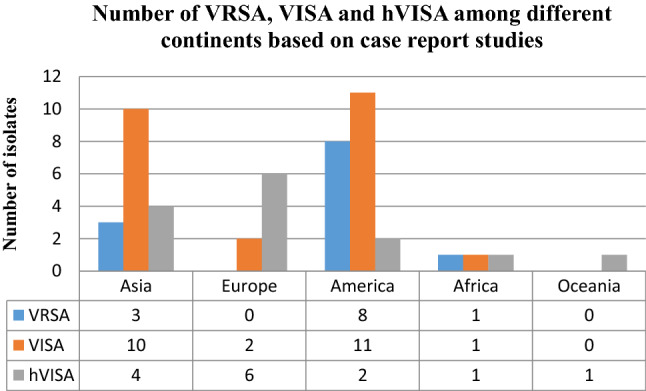
Vancomycin-resistant Staphylococcus aureus (VRSA), Vancomycin-intermediate S. aureus (VISA) and heterogeneous VISA (hVISA) are subject to vancomycin treatment failure. The aim of the present study was to determine their precise prevalence and investigate prevalence variability depending on different years and locations. Several international databases including Medline (PubMed), Embase and Web of Sciences were searched (data from 1997 to 2019) to identify studies that addressed the prevalence of VRSA, VISA and hVISA among human clinical isolates around the world. Subgroup analyses and meta-regression were conducted to indicate potential source of variation. Publication bias was assessed using Egger's test. Statistical analyses were conducted using STATA software (version 14.0). Data analysis showed that VRSA, VISA and hVISA isolates were reported in 23, 50 and 82 studies, with an overall prevalence of 1.5% among 5855 S. aureus isolates, 1.7% among 22,277 strains and 4.6% among 47,721 strains, respectively. The overall prevalence of VRSA, VISA, and hVISA before 2010 was 1.2%, 1.2%, and 4%, respectively, while their prevalence after this year has reached 2.4%, 4.3%, and 5.3%. The results of this study showed that the frequency of VRSA, VISA and hVISA after 2010 represent a 2.0, 3.6 and 1.3-fold increase over prior years. In a subgroup analysis of different strain origins, the highest frequency of VRSA (3.6%) and hVISA (5.2%) was encountered in the USA while VISA (2.1%) was more prevalent in Asia. Meta-regression analysis showed significant increasing of VISA prevalence in recent years (p value ≤ 0.05). Based on the results of case reports (which were not included in the calculations mentioned above), the numbers of VRSA, VISA and hVISA isolates were 12, 24 and 14, respectively, among different continents. Since the prevalence of VRSA, VISA and hVISA has been increasing in recent years (especially in the Asian and American continents), rigorous monitoring of vancomycin treatment, it's the therapeutic response and the definition of appropriate control guidelines depending on geographical regions is highly recommended and essential to prevent the further spread of vancomycin-resistant S. aureus.
耐万古霉素金黄色葡萄球菌(VRSA)、万古霉素中介金黄色葡萄球菌(VISA)和异质性 VISA(hVISA)对万古霉素治疗失败。本研究的目的是确定它们的确切流行率,并研究不同年份和地点的流行率变化。检索了包括 Medline(PubMed)、Embase 和 Web of Sciences 在内的多个国际数据库(数据来自 1997 年至 2019 年),以确定全球人类临床分离株中 VRSA、VISA 和 hVISA 流行率的研究。进行了亚组分析和荟萃回归分析,以指示潜在的变异来源。使用 Egger 检验评估发表偏倚。使用 STATA 软件(版本 14.0)进行统计分析。数据分析显示,在 23 项、50 项和 82 项研究中报告了 VRSA、VISA 和 hVISA 分离株,在 5855 株金黄色葡萄球菌分离株中总体流行率为 1.5%,在 22277 株菌株中为 1.7%,在 47721 株菌株中为 4.6%。2010 年之前 VRSA、VISA 和 hVISA 的总体流行率分别为 1.2%、1.2%和 4%,而此后的流行率已分别达到 2.4%、4.3%和 5.3%。本研究结果表明,2010 年后 VRSA、VISA 和 hVISA 的频率分别比前几年增加了 2.0、3.6 和 1.3 倍。在不同菌株来源的亚组分析中,美国发现 VRSA(3.6%)和 hVISA(5.2%)的频率最高,而亚洲 VISA(2.1%)更为普遍。荟萃回归分析显示,近年来 VISA 流行率呈显著上升趋势(p 值≤0.05)。基于病例报告的结果(未包含在上述计算中),在不同大陆,VRSA、VISA 和 hVISA 分离株的数量分别为 12、24 和 14。由于 VRSA、VISA 和 hVISA 的流行率近年来一直在上升(尤其是在亚洲和美洲大陆),强烈建议严格监测万古霉素治疗、治疗反应,并根据地理区域制定适当的控制指南,以防止耐万古霉素金黄色葡萄球菌的进一步传播。