Kloprogge Frank, Mwandumba Henry C, Banda Gertrude, Kamdolozi Mercy, Shani Doris, Corbett Elizabeth L, Kontogianni Nadia, Ward Steve, Khoo Saye H, Davies Geraint R, Sloan Derek J
Institute for Global Health, University College London, London, United Kingdom.
Malawi Liverpool Wellcome Trust Clinical Research Programme, Blantyre, Malawi.
Open Forum Infect Dis. 2020 Jun 6;7(7):ofaa218. doi: 10.1093/ofid/ofaa218. eCollection 2020 Jul.
This study aims to explore relationships between baseline demographic covariates, plasma antibiotic exposure, sputum bacillary load, and clinical outcome data to help improve future tuberculosis (TB) treatment response predictions.
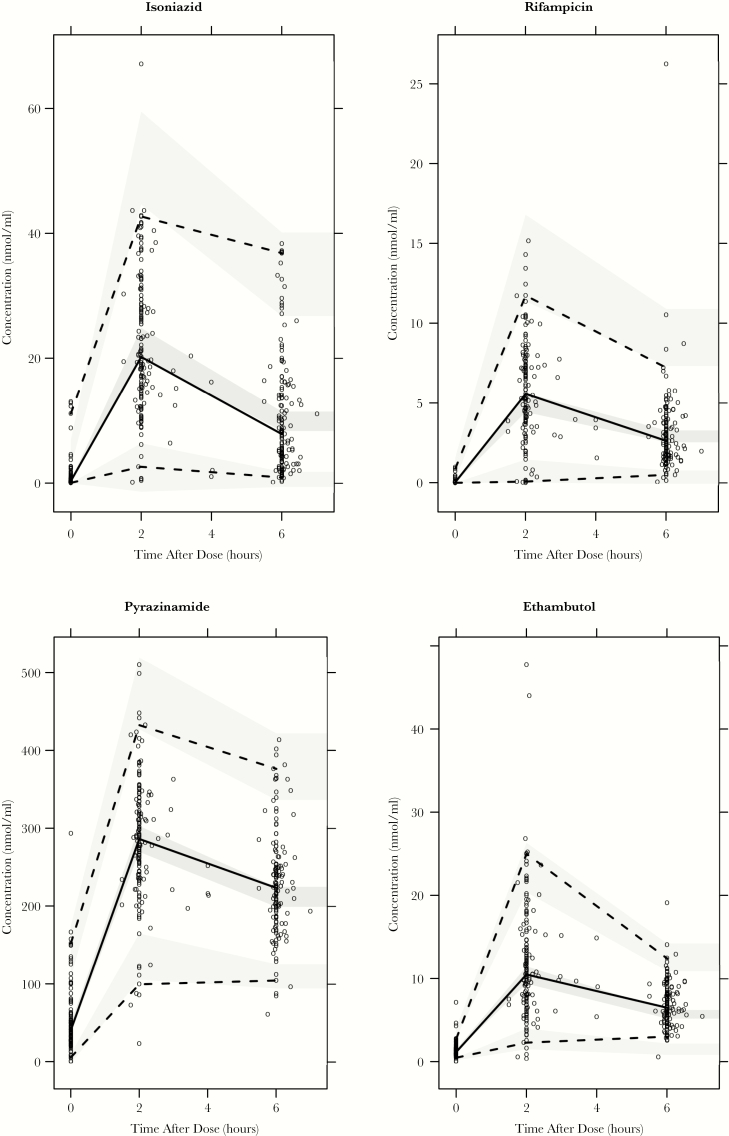
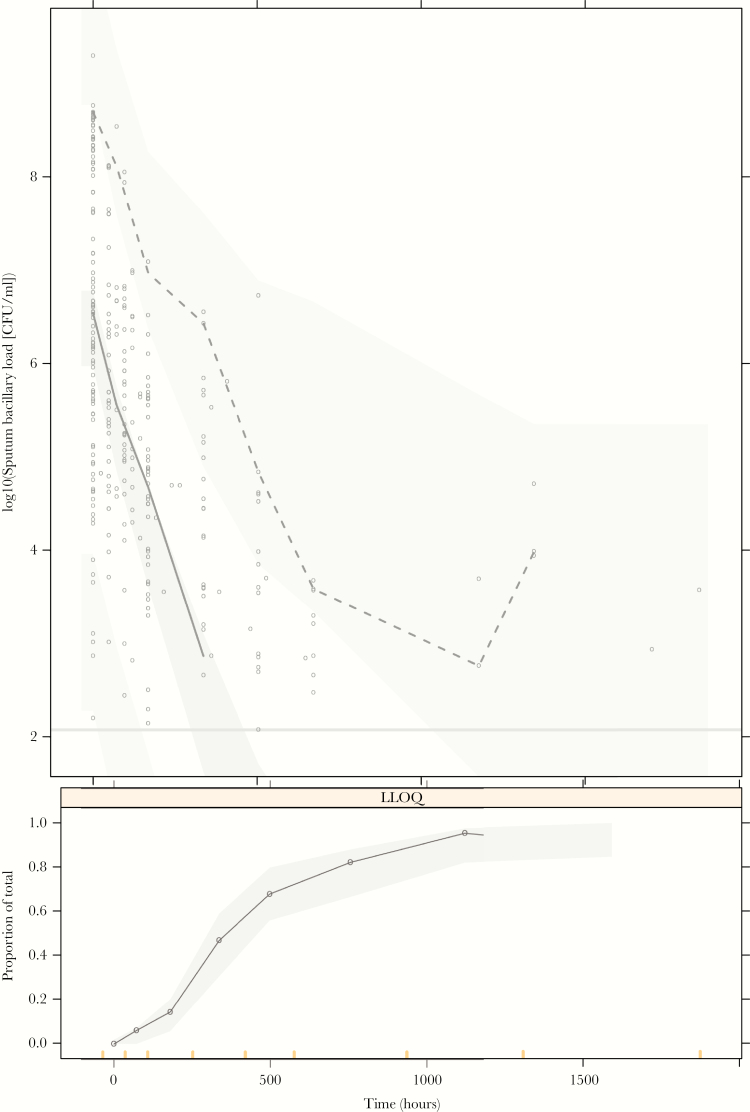
Data were available from a longitudinal cohort study in Malawian drug-sensitive TB patients on standard therapy, including steady-state plasma antibiotic exposure (154 patients), sputum bacillary load (102 patients), final outcome (95 patients), and clinical details. Population pharmacokinetic and pharmacokinetic-pharmacodynamic models were developed in the software package NONMEM. Outcome data were analyzed using univariate logistic regression and Cox proportional hazard models in R, a free software for statistical computing.
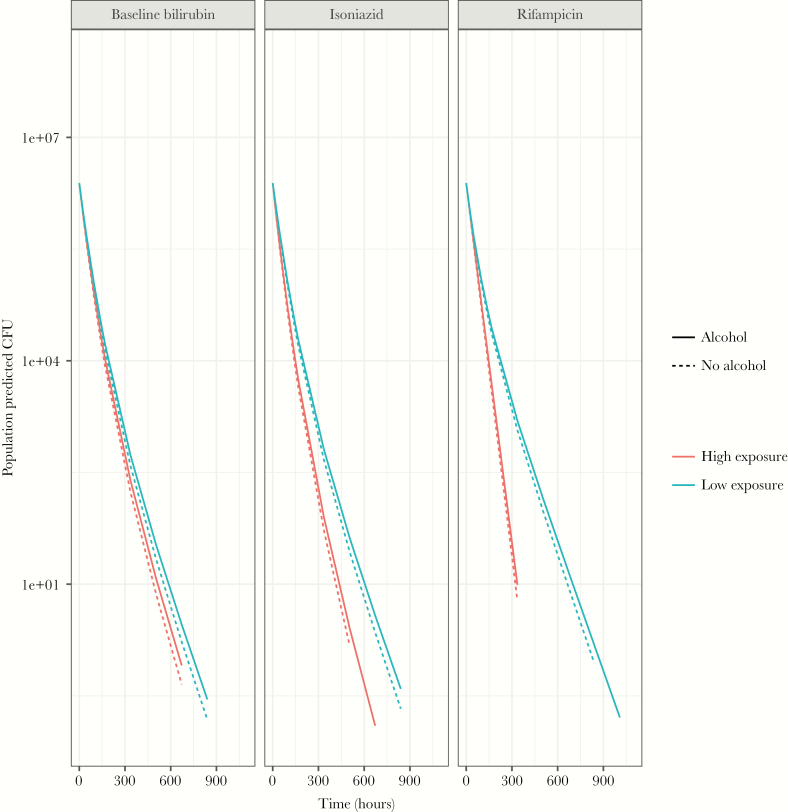
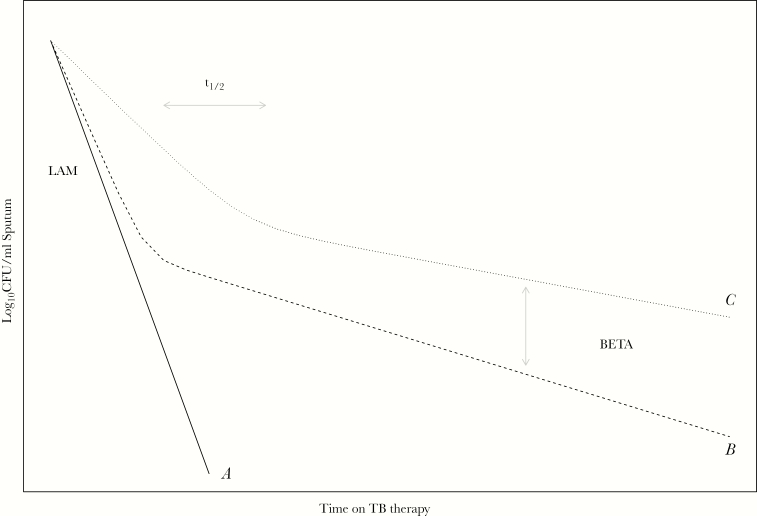
Higher isoniazid exposure correlated with increased bacillary killing in sputum (.01). Bacillary killing in sputum remained fast, with later progression to biphasic decline, in patients with higher rifampicin area under the curve (AUC) (01). Serial sputum colony counting negativity at month 2 (05), isoniazid (.05), isoniazid /minimum inhibitory concentration ([MIC] 01), and isoniazid AUC/MIC (01) correlated with treatment success but not with remaining free of TB. Slower bacillary killing (05) and earlier progression to biphasic bacillary decline (01) both correlate with treatment failure. Posttreatment recurrence only correlated with slower bacillary killing (05).
Patterns of early bacillary clearance matter. Static measurements such as month 2 sputum conversion and pharmacokinetic parameters such as /MIC and AUC/MIC were predictive of treatment failure, but modeling of quantitative longitudinal data was required to assess the risk of recurrence. Pooled individual patient data analyses from larger datasets are needed to confirm these findings.
本研究旨在探索基线人口统计学协变量、血浆抗生素暴露、痰液细菌载量和临床结局数据之间的关系,以帮助改进未来结核病(TB)治疗反应预测。
数据来自一项针对马拉维接受标准治疗的药物敏感型结核病患者的纵向队列研究,包括稳态血浆抗生素暴露(154例患者)、痰液细菌载量(102例患者)、最终结局(95例患者)和临床细节。在软件包NONMEM中建立了群体药代动力学和药代动力学-药效学模型。使用R语言(一种免费的统计计算软件)中的单变量逻辑回归和Cox比例风险模型对结局数据进行分析。
较高的异烟肼暴露与痰液中细菌杀灭增加相关(P=0.01)。曲线下面积(AUC)较高的利福平患者痰液中的细菌杀灭速度仍然较快,随后进展为双相下降(P=0.01)。第2个月连续痰液菌落计数阴性(P=0.05)、异烟肼(P=0.05)、异烟肼/最低抑菌浓度([MIC],P=0.01)和异烟肼AUC/MIC(P=0.01)与治疗成功相关,但与结核病未复发无关。较慢的细菌杀灭速度(P=0.05)和较早进展为双相细菌下降(P=0.01)均与治疗失败相关。治疗后复发仅与较慢的细菌杀灭速度相关(P=0.05)。
早期细菌清除模式很重要。诸如第2个月痰液转阴等静态测量以及诸如/C和AUC/M等药代动力学参数可预测治疗失败,但需要对定量纵向数据进行建模以评估复发风险。需要从更大的数据集中进行汇总个体患者数据分析以证实这些发现。