Benefits Division, California Department of Health Care Services, Sacramento, California, United States of America.
School of Agriculture and Food Sciences, Faculty of Science, The University of Queensland, Brisbane, Queensland, Australia.
PLoS One. 2020 Aug 6;15(8):e0236877. doi: 10.1371/journal.pone.0236877. eCollection 2020.
To identify current maternal and infant predictors of infant mortality, including maternal sociodemographic and economic status, maternal perinatal smoking and obesity, mode of delivery, and infant birthweight and gestational age.
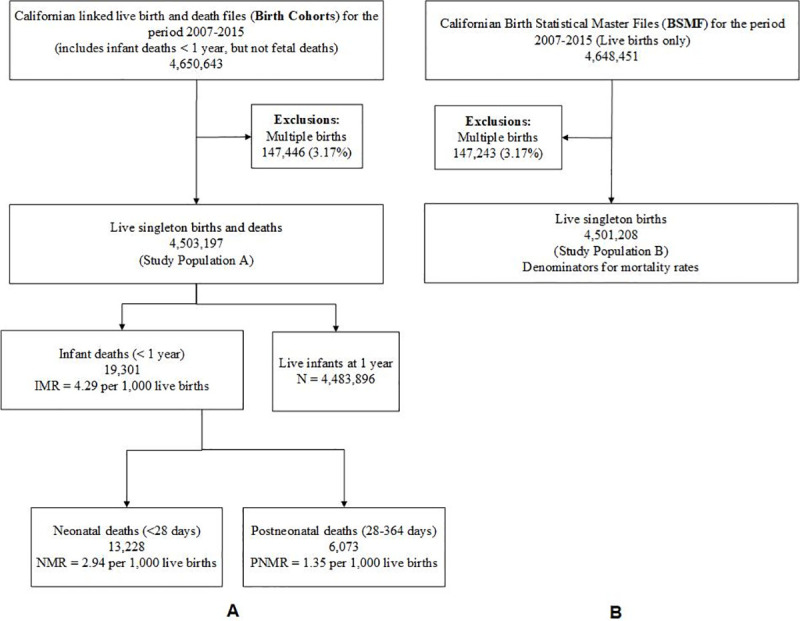
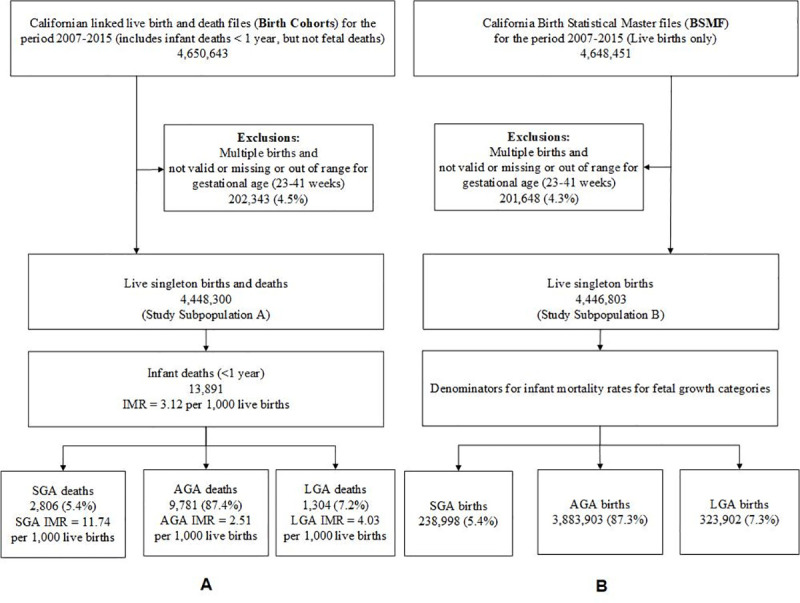
This retrospective study analyzed data from the linked birth and infant death files (birth cohort) and live births from the Birth Statistical Master files (BSMF) in California compiled by the California Department of Public Health for 2007-2015. The birth cohort study comprised 4,503,197 singleton births including 19,301 infant deaths during the nine-year study period. A subpopulation to study fetal growth consisted of 4,448,300 birth cohort records including 13,891 infant deaths.
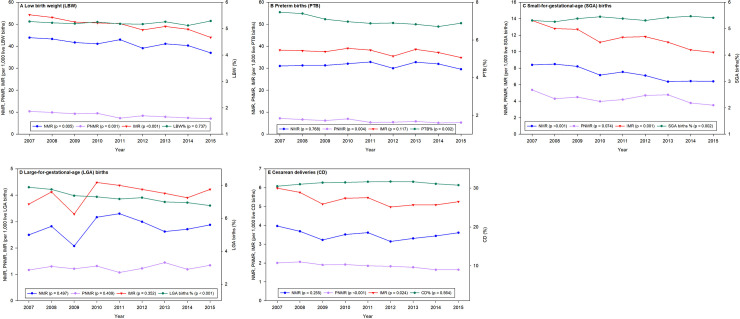
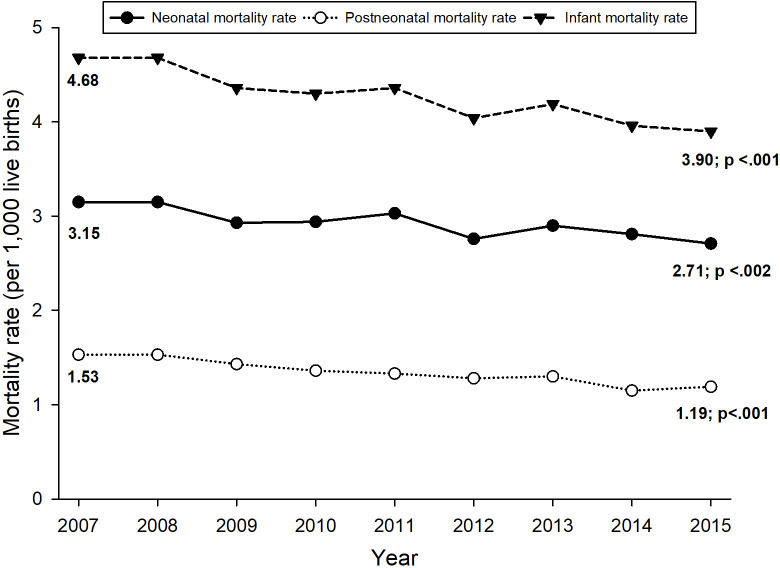
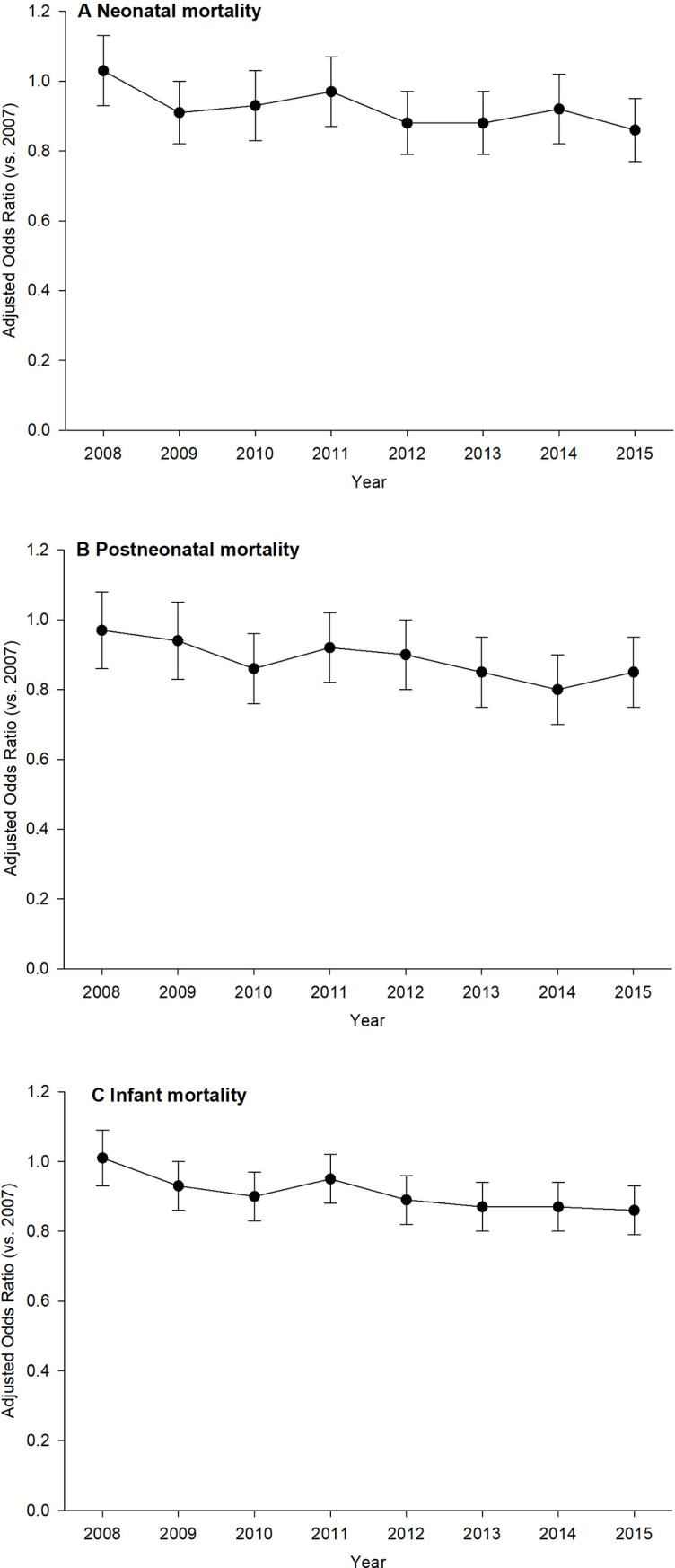
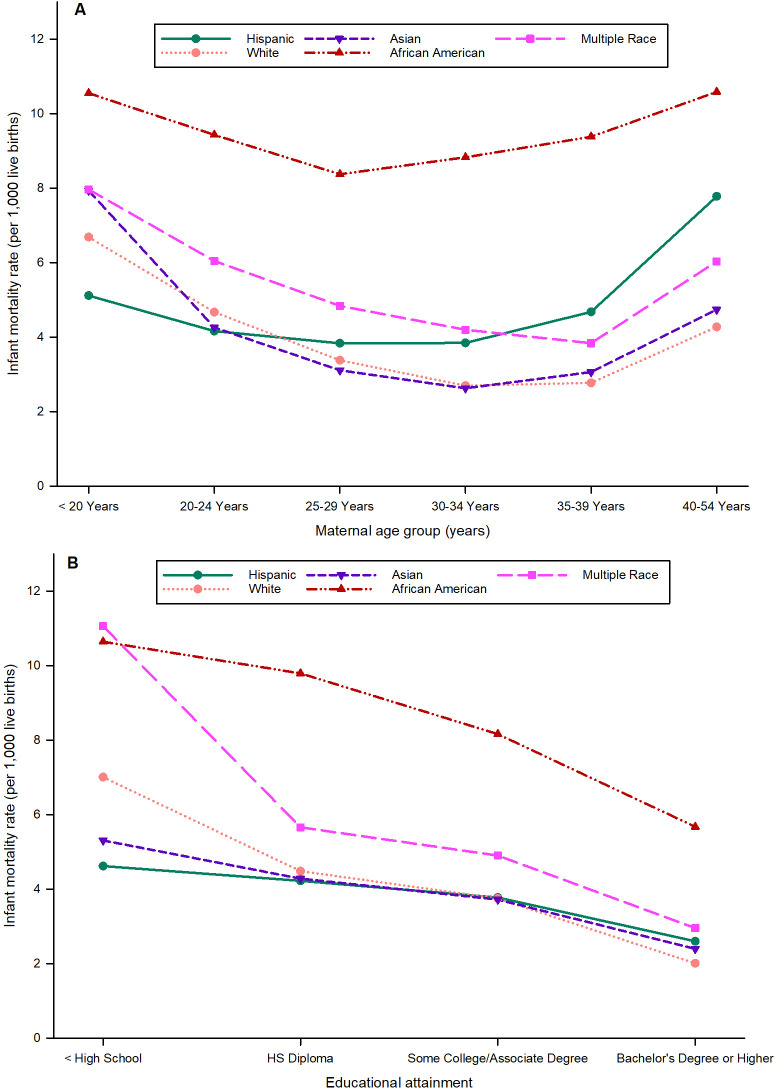
The infant mortality rate (IMR) for singleton births decreased linearly (p <0.001) from 4.68 in 2007 to 3.90 (per 1,000 live births) in 2015. However, significant disparities in IMR were uncovered in different population groups depending upon maternal sociodemographic and economic characteristics and maternal characteristics during pregnancy. Children of African American women had almost twice the risk of infant mortality when compared with children of White women (AOR 2.12; 95% CI, 1.98-2.27; p<0.001). Infants of women with Bachelor's degrees or higher were 89% less likely to die (AOR 1.89; 95% CI, 1.76-2.04; p<0.001) when compared to infants of women with education less than high school. Infants of maternal smokers were 75% more likely to die (AOR 1.75; 95% CI, 1.58-1.93; p<0.001) than infants of nonsmokers. Infants of women who were overweight and obese during pregnancy accounted for 55% of IMR over all women in the study. More than half of the infant deaths were to children of women with lower socioeconomic status; infants of WIC participants were 59% more likely to die (AOR 1.59; 95% CI, 1.52-1.67; p<0.001) than infants of non-WIC participants. With respect to infant predictors, infants born with LBW or PTB were more than six times (AOR 6.29; 95% CI, 5.90-6.70; p<0.001) and almost four times (AOR 3.95; 95% CI, 3.73-4.19; p<0.001) more likely to die than infants who had normal births, respectively. SGA and LGA infants were more than two times (AOR 2.03; 95% CI, 1.92-2.15; p<0.001) and 41% (AOR 1.41; 95% CI, 1.32-1.52; p<0.001) more likely to die than AGA infants, respectively.
While the overall IMR in California is declining, wide disparities in death rates persist in different groups, and these disparities are increasing. Our data indicate that maternal sociodemographic and economic factors, as well as maternal prepregnancy obesity and smoking during pregnancy, have a prominent effect on IMR though no causality can be inferred with the current data. These predictors are not typically addressed by direct medical care. Infant factors with a major effect on IMR are birthweight and gestational age-predictors that are addressed by active medical services. The highest value interventions to reduce IMR may be social and public health initiatives that mitigate disparities in sociodemographic, economic and behavioral risks for mothers.
确定当前影响婴儿死亡率的母婴预测因素,包括产妇社会人口经济学状况、产妇围产期吸烟和肥胖、分娩方式以及婴儿出生体重和胎龄。
本回顾性研究分析了加利福尼亚州公共卫生部汇编的 2007 年至 2015 年出生和婴儿死亡档案(出生队列)和活产儿出生统计主文件(BSMF)中的数据。出生队列研究包括 4503197 例单胎分娩,在九年研究期间有 19301 例婴儿死亡。一个研究胎儿生长的子人群包括 4448300 例出生队列记录,其中有 13891 例婴儿死亡。
2007 年至 2015 年,单胎出生的婴儿死亡率(IMR)呈线性下降(p<0.001),从 4.68 降至 3.90(每 1000 例活产儿)。然而,根据产妇社会人口经济学特征和妊娠期间产妇特征,不同人群组的 IMR 存在显著差异。与白人妇女的婴儿相比,非裔美国妇女的婴儿死亡风险几乎高出两倍(优势比 2.12;95%置信区间,1.98-2.27;p<0.001)。与教育程度低于高中的妇女相比,拥有学士学位或更高学历的妇女的婴儿死亡风险降低了 89%(优势比 1.89;95%置信区间,1.76-2.04;p<0.001)。与不吸烟的妇女相比,吸烟的产妇的婴儿死亡风险增加了 75%(优势比 1.75;95%置信区间,1.58-1.93;p<0.001)。妊娠期间超重和肥胖的妇女占研究中所有妇女 IMR 的 55%。超过一半的婴儿死亡是母亲社会经济地位较低的儿童;WIC 参与者的婴儿死亡风险增加 59%(优势比 1.59;95%置信区间,1.52-1.67;p<0.001),而非 WIC 参与者的婴儿。就婴儿预测因素而言,出生体重低或早产的婴儿死亡风险增加超过六倍(优势比 6.29;95%置信区间,5.90-6.70;p<0.001),几乎四倍(优势比 3.95;95%置信区间,3.73-4.19;p<0.001),分别比正常出生的婴儿更容易死亡。SGA 和 LGA 婴儿的死亡风险分别增加两倍(优势比 2.03;95%置信区间,1.92-2.15;p<0.001)和 41%(优势比 1.41;95%置信区间,1.32-1.52;p<0.001),而 AGA 婴儿的死亡风险较低。
虽然加利福尼亚州的总体 IMR 正在下降,但不同群体的死亡率仍存在很大差异,而且这些差异还在增加。我们的数据表明,产妇社会人口经济学特征以及产妇妊娠前肥胖和吸烟对 IMR 有显著影响,但不能从当前数据中推断出因果关系。这些预测因素通常不会通过直接的医疗护理来解决。对 IMR 有重大影响的婴儿因素是出生体重和胎龄-通过积极的医疗服务来解决的预测因素。降低 IMR 的最高价值干预措施可能是减轻母亲的社会人口、经济和行为风险方面的社会和公共卫生举措。