Kumar Lakshmi, Kumar Kalyan, Sandhya Sai, Koshy Deepa M, Ramamurthi Kruthika P, Rajan Sunil
Department of Anaesthesiology, Amrita Institute of Medical Sciences, Amrita Vishwa Vidyapeetham, Kochi, Kerala, India.
Indian J Anaesth. 2020 Jul;64(7):599-604. doi: 10.4103/ija.IJA_401_20. Epub 2020 Jul 1.
Minimally invasive and robotic surgeries need lesser fluid replacement but the role of restricted fluids in robotic surgeries other than prostatic surgeries has not been clearly defined. Our primary aim was to evaluate the effects of a restrictive fluid regimen versus a liberal policy on intra-operative lactate in robotic colorectal surgery. Secondary outcomes were need for vasopressors, extubation on table, post-operative renal functions and length of ICU (LOICU) stay.
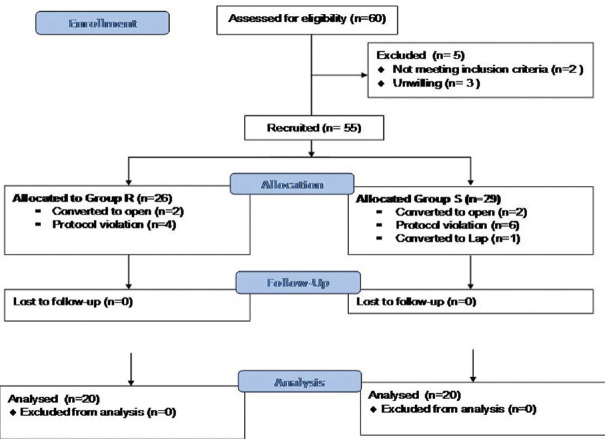
American society of anaesthesiologists (ASA) physical status I-II patients scheduled for robot-assisted colorectal surgery were randomised into one of two groups, receiving either 2 mL/kg/h (Group R) or 4mL/kg/h, (group L). Fluid boluses of 250 ml were administered if mean arterial pressure (MAP) <65 mmHg or urine output <0.5 ml/kg/h. Norepinephrine was added for the blood pressure after 2 fluid boluses. Surgical field was assessed by modified Boezaart's scale and surgeon satisfaction by Likert scale.
Demographics and baseline renal functions were comparable. Adjusted intra-operative lactate at 2 h, 4 h, and 6 h and need for noradrenaline and post-operative creatinine were similar. One patient in the group L was ventilated due to hypothermia. The field was better at the 4 h in group R and comparable at other time points. The LOICU stay was longer in Group L.
The use of restrictive fluid strategy of 2 mL/kg/h (group R) does not increase lactate levels or creatinine, improves surgical field at 4 h and shortens ICU stay in comparison to a liberal 4 mL/kg/h (group L) in robotic colorectal surgery.
微创和机器人手术需要较少的液体补充,但除前列腺手术外,限制液体在机器人手术中的作用尚未明确界定。我们的主要目的是评估在机器人结直肠手术中,限制性液体方案与宽松方案对术中乳酸水平的影响。次要结果包括血管升压药的使用需求、术中拔管情况、术后肾功能以及重症监护病房(ICU)住院时间。
计划接受机器人辅助结直肠手术的美国麻醉医师协会(ASA)身体状况I-II级患者被随机分为两组,分别接受2 mL/kg/h(R组)或4 mL/kg/h(L组)的补液。如果平均动脉压(MAP)<65 mmHg或尿量<0.5 ml/kg/h,则给予250 ml液体冲击量。在两次液体冲击后,若血压仍低则添加去甲肾上腺素。采用改良的Boezaart量表评估手术视野,采用Likert量表评估外科医生的满意度。
人口统计学和基线肾功能具有可比性。2小时、4小时和6小时的调整后术中乳酸水平、去甲肾上腺素的使用需求以及术后肌酐水平相似。L组有1例患者因体温过低需要机械通气。R组在4小时时手术视野更好,其他时间点相当。L组的ICU住院时间更长。
与宽松的4 mL/kg/h(L组)相比,在机器人结直肠手术中采用2 mL/kg/h的限制性液体策略(R组)不会增加乳酸水平或肌酐水平,可在4小时时改善手术视野并缩短ICU住院时间。