Anjara S G, Bonetto C, Van Bortel T, Brayne C
Cambridge Institute of Public Health, University of Cambridge, School of Clinical Medicine, Cambridge Biomedical Campus, Forvie Site, Robinson Way, Box 113, Cambridge, CB2 0SR UK.
Department of Neurosciences, Biomedicine and Movement Sciences, University of Verona, Piazzale L.A. Scuro 10, 37134 Verona, Italy.
Int J Ment Health Syst. 2020 Aug 10;14:62. doi: 10.1186/s13033-020-00397-0. eCollection 2020.
This study explores the factor structure of the Indonesian version of the GHQ-12 based on several theoretical perspectives and determines the threshold for optimum sensitivity and specificity. Through a focus group discussion, we evaluate the practicality of the GHQ-12 as a screening tool for mental health problems among adult primary care patients in Indonesia.
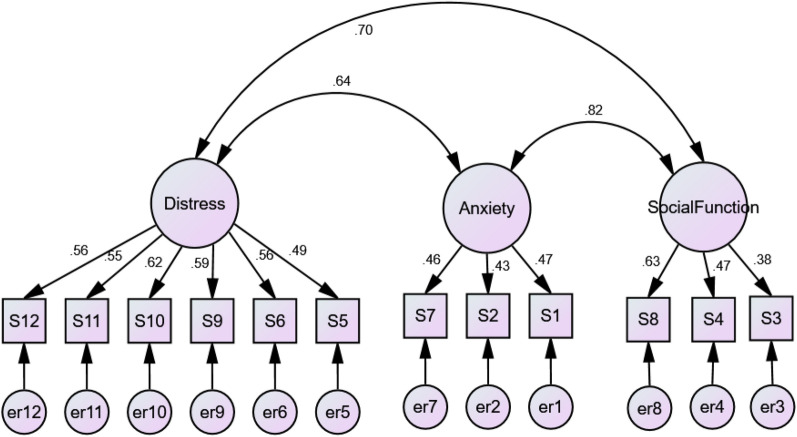
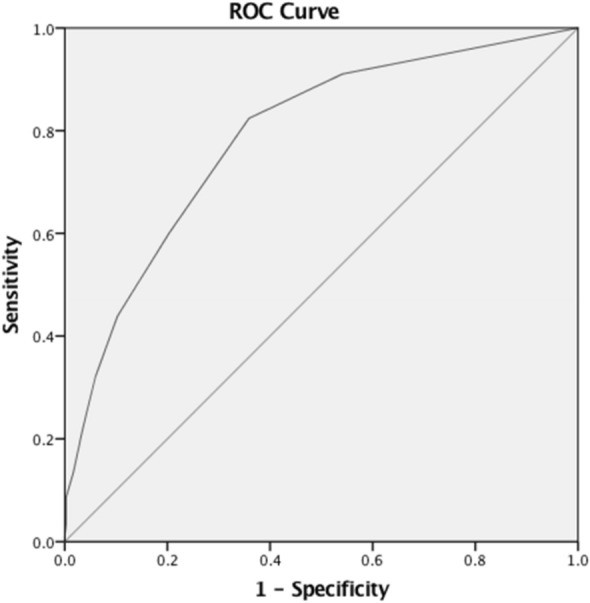
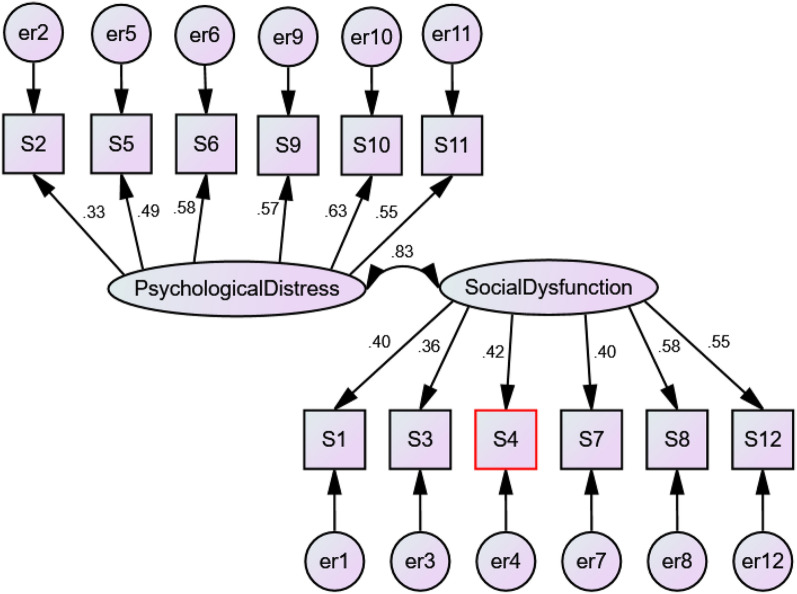
This is a prospective study exploring the construct validity, criterion validity and reliability of the GHQ-12, conducted with 676 primary care patients attending 28 primary care clinics randomised for participation in the study. Participants' GHQ-12 scores were compared with their psychiatric diagnosis based on face-to-face clinical interviews with GPs using the CIS-R. Exploratory and Confirmatory Factor Analyses determined the construct validity of the GHQ-12 in this population. The appropriate threshold score of the GHQ-12 as a screening tool in primary care was determined using the receiver operating curve. Prior to data collection, a focus group discussion was held with research assistants who piloted the screening procedure, GPs, and a psychiatrist, to evaluate the practicality of embedding screening within the routine clinic procedures.
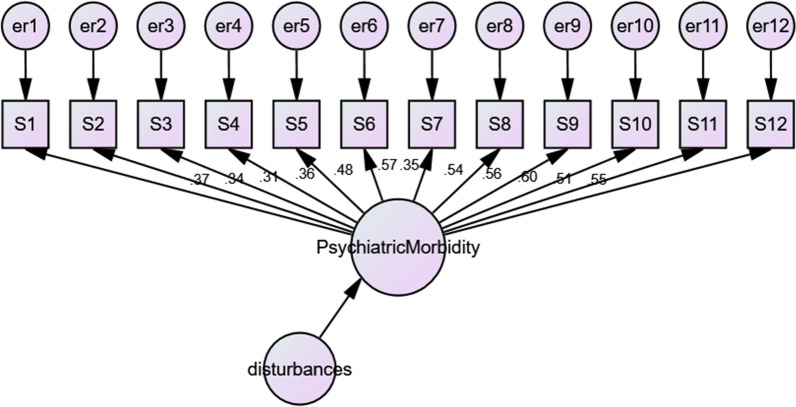
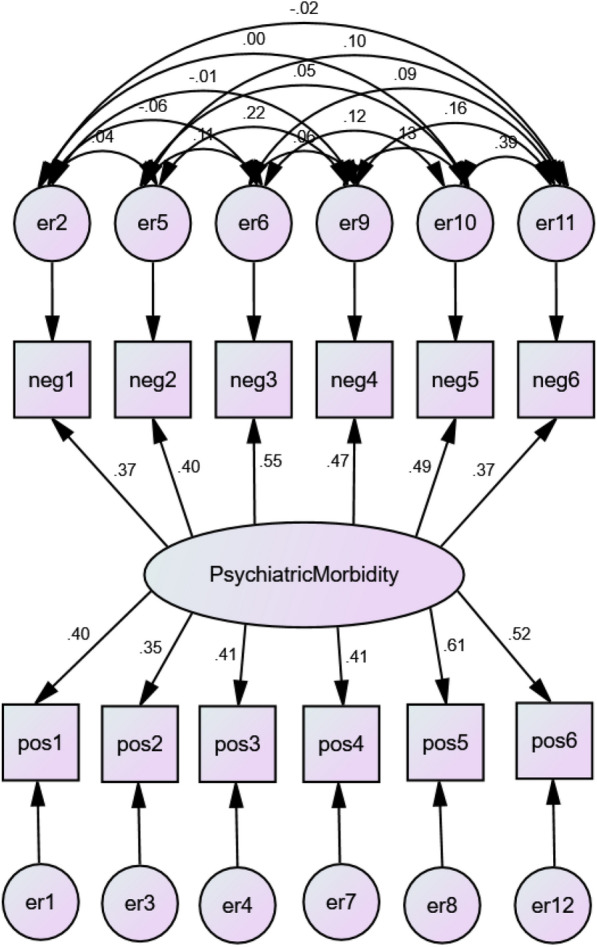
Of all primary care patients attending the clinics during the recruitment period, 26.7% agreed to participate (676/2532 consecutive patients approached). Their median age was 46 (range 18-82 years); 67% were women. The median GHQ-12 score for our primary care sample was 2, with an interquartile range of 4. The internal consistency of the GHQ-12 was good (Cronbach's α = 0.76). Four factor structures were fitted on the data. The GHQ-12 was found to best fit a one-dimensional model, when response bias is taken into consideration. Results from the ROC curve indicated that the GHQ-12 is 'fairly accurate' when discriminating primary care patients with indication of mental disorders from those without, with average AUC of 0.78. The optimal threshold of the GHQ-12 was either 1/2 or 2/3 point depending on the intended utility, with a Positive Predictive Value of 0.68 to 0.73 respectively. The screening procedure was successfully embedded into routine patient flow in the 28 clinics.
The Indonesian version of the GHQ-12 could be used to screen primary care patients at high risk of mental disorders although with significant false positives if reasonable sensitivity is to be achieved. While it involves additional administrative burden, screening may help identify future users of mental health services in primary care that the country is currently expanding.
本研究基于多种理论视角探讨了印度尼西亚版GHQ - 12的因子结构,并确定了最佳敏感性和特异性的阈值。通过焦点小组讨论,我们评估了GHQ - 12作为印度尼西亚成年初级保健患者心理健康问题筛查工具的实用性。
这是一项前瞻性研究,旨在探讨GHQ - 12的结构效度、效标效度和信度,研究对象为随机参与该研究的28家初级保健诊所的676名初级保健患者。根据使用CIS - R对全科医生进行的面对面临床访谈得出的精神病诊断结果,对参与者的GHQ - 12得分进行比较。探索性因子分析和验证性因子分析确定了GHQ - 12在该人群中的结构效度。使用受试者工作特征曲线确定了GHQ - 12作为初级保健筛查工具的合适阈值分数。在数据收集之前,与参与筛查程序试点的研究助理、全科医生和一名精神科医生进行了焦点小组讨论,以评估将筛查纳入常规门诊程序的实用性。
在招募期间到诊所就诊的所有初级保健患者中,26.7%同意参与(共接触2532名连续患者,其中676名同意)。他们的年龄中位数为46岁(范围18 - 82岁);67%为女性。我们初级保健样本的GHQ - 12得分中位数为2,四分位距为4。GHQ - 12的内部一致性良好(Cronbach's α = 0.76)。对数据拟合了四种因子结构。当考虑反应偏倚时,发现GHQ - 12最适合一维模型。ROC曲线结果表明,在区分有精神障碍迹象的初级保健患者和无精神障碍迹象的患者时,GHQ - 12“相当准确”,平均AUC为0.78。根据预期用途,GHQ - 12的最佳阈值为1/2或2/3分,阳性预测值分别为0.68至0.73。筛查程序成功纳入了28家诊所的常规患者流程。
印度尼西亚版的GHQ - 12可用于筛查有精神障碍高风险的初级保健患者,不过如果要实现合理的敏感性,则会有显著的假阳性。虽然筛查会带来额外的管理负担,但它可能有助于识别该国目前正在扩大的初级保健中未来的心理健康服务使用者。