Dial Brian L, Esposito Valentine R, Catanzano Anthony A, Fitch Robert D, Lark Robert K
yDuke University Medical Center, Durham, NC, USA.
University of Washington, Seattle, WA, USA.
Global Spine J. 2021 Sep;11(7):1076-1082. doi: 10.1177/2192568220941456. Epub 2020 Aug 17.
Retrospective study.
Previous studies have demonstrated that increased implant density (ID) results in improved coronal deformity correction. However, low-density constructs with strategically placed fixation points may achieve similar coronal correction. The purpose of this study was to identify key zones along the spinal fusion where high ID statistically correlated to improved coronal deformity correction. Our hypothesis was that high ID within the periapical zone would not be associated with increased percent Cobb correction.
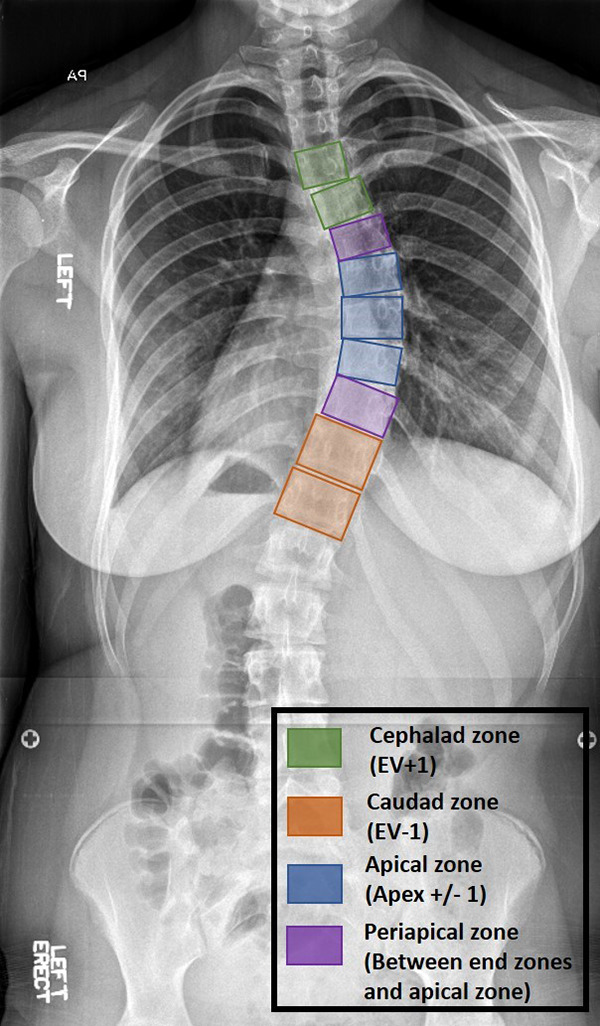
We identified patients with Lenke type 1 curves with a minimum 2-year follow up. The instrumented vertebral levels were divided into 4 zones: (1) cephalad zone, (2) caudal zone, (3) apical zone, and (4) periapical zone. High and low percent Cobb correction groups were compared, high percent Cobb group was defined as percent correction >67%. Total ID, total concave ID, total convex ID, and ID within each zone of the curve were compared between the groups. A multivariable analysis was performed to identify independent predictors for coronal correction. Subsequently increased and decreased thoracic kyphosis (TK) groups were compared, increased TK was defined as post-operative TK being larger than preoperative TK and decreased TK was defined as post-operative TK being less than preoperative TK.
The cohort included 68 patients. The high percent Cobb group compared with the low percent Cobb group had significantly greater ID for the entire construct, the total concave side, the total convex side, the apical convex zone, the periapical zone, and the cephalad concave zone. The high percent Cobb group had greater pedicle screw density for the total construct, total convex side, and total concave side. In the multivariate model ID and pedicle screw density remained significant for percent Cobb correction. Ability to achieve coronal balance was not statistically correlated to ID ( = .78).
Increased ID for the entire construct, the entire convex side, the entire concave side, and within each spinal zone was associated with improved percent Cobb correction. The ability to achieve coronal balance was not statistically influence by ID. The results of this study support that increasing ID along the entire length of the construct improves percent Cobb correction.
回顾性研究。
既往研究表明,增加植入物密度(ID)可改善冠状面畸形矫正效果。然而,具有策略性放置固定点的低密度结构可能实现类似的冠状面矫正。本研究的目的是确定脊柱融合沿线的关键区域,在这些区域高ID与改善冠状面畸形矫正具有统计学相关性。我们的假设是根尖周区域内的高ID与增加的Cobb角矫正百分比无关。
我们确定了至少随访2年的Lenke 1型曲线患者。将植入器械的椎体节段分为4个区域:(1)头侧区域,(2)尾侧区域,(3)顶椎区域,和(4)根尖周区域。比较高Cobb角矫正百分比组和低Cobb角矫正百分比组,高Cobb角组定义为矫正百分比>67%。比较两组之间的总ID、总凹侧ID、总凸侧ID以及曲线各区域内的ID。进行多变量分析以确定冠状面矫正的独立预测因素。随后比较胸椎后凸(TK)增加组和减少组,增加的TK定义为术后TK大于术前TK,减少的TK定义为术后TK小于术前TK。
该队列包括68例患者。高Cobb角百分比组与低Cobb角百分比组相比,整个结构、总凹侧、总凸侧、顶椎凸侧区域、根尖周区域和头侧凹侧区域的ID显著更高。高Cobb角百分比组在整个结构、总凸侧和总凹侧的椎弓根螺钉密度更高。在多变量模型中,ID和椎弓根螺钉密度对Cobb角矫正百分比仍具有显著意义。实现冠状面平衡的能力与ID无统计学相关性(P = 0.78)。
整个结构、整个凸侧、整个凹侧以及每个脊柱区域内ID的增加与Cobb角矫正百分比的改善相关。实现冠状面平衡的能力不受ID的统计学影响。本研究结果支持在整个结构长度上增加ID可改善Cobb角矫正百分比。