Section of Cardiovascular Medicine, Department of Medicine, Columbia University Irving Medical Center, New York, NY; Center for Outcomes Research and Evaluation, Yale-New Haven Hospital, New Haven, Conn; Cardiovascular Research Foundation, New York, NY.
Department of Internal Medicine, Geriatrics Section, and the Program on Aging.
Am J Med. 2021 Jan;134(1):95-103. doi: 10.1016/j.amjmed.2020.07.020. Epub 2020 Aug 14.
Oldest-old patients (≥85 years) constitute half the acute myocardial infarction hospitalizations among older adults and more commonly have atypical presentation, under-treatment, and functional impairments. Yet this group has not been well characterized. We characterized differences in presentation, functional impairments, treatments, health status, and mortality among middle-old (75-84 years) and oldest-old patients with myocardial infarction.
We analyzed data from the ComprehenSIVe Evaluation of Risk Factors in Older Patients with AMI (SILVER-AMI) study that enrolled 3041 patients ≥75 years of age from 94 hospitals across the US between 2013 and 2016. We performed Cox proportional hazards regression to examine the association between the oldest-old (n = 831) and middle-old (n = 2210) age categories with postdischarge 6-month case fatality rate adjusting for sociodemographic and clinical variables, and mobility impairment.
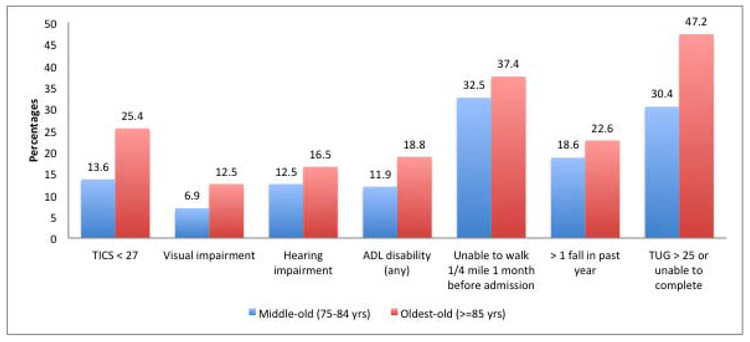
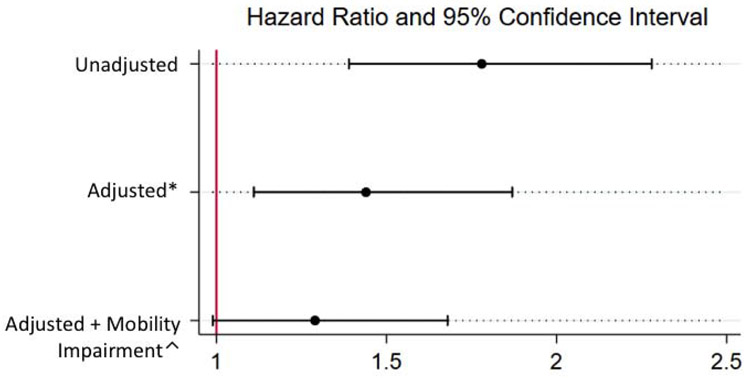
The oldest-old were less likely to present with chest pain (52.7% vs 57.7%) as their primary symptom or to receive coronary revascularization (58.1% vs 71.8) (P < .01 for both). The oldest-old were more likely to have functional impairments and had higher 6-month mortality compared with the middle-old patients (hazard ratio 1.78, 95% confidence interval, 1.39-2.28). This association was substantially attenuated after adjusting for mobility impairment (hazard ratio 1.29, confidence interval, 0.99-1.68).
There is considerable heterogeneity in presentation, treatment, and outcomes among older patients with myocardial infarction. Mobility impairment, a marker for frailty, modifies the association between advanced age and treatments as well as outcomes.
最年长的老年患者(≥85 岁)占老年人群中急性心肌梗死住院患者的一半,他们更常出现非典型表现、治疗不足和功能障碍。然而,这一群体尚未得到充分描述。我们描述了具有心肌梗死的中老年(75-84 岁)和最年长老年患者在表现、功能障碍、治疗、健康状况和死亡率方面的差异。
我们分析了 2013 年至 2016 年期间来自美国 94 家医院的 3041 名年龄≥75 岁的 ComprehenSIVe Evaluation of Risk Factors in Older Patients with AMI(SILVER-AMI)研究的数据。我们使用 Cox 比例风险回归分析,根据社会人口统计学和临床变量以及移动障碍,检查最年长老年(n=831)和中老年(n=2210)年龄组与出院后 6 个月病死率之间的关联。
最年长老年患者作为主要症状就诊时更可能出现胸痛(52.7% vs. 57.7%)或接受冠状动脉血运重建(58.1% vs. 71.8%)(均 P<.01)。与中老年患者相比,最年长老年患者的功能障碍更常见,且 6 个月死亡率更高(风险比 1.78,95%置信区间,1.39-2.28)。在调整移动障碍后,这种关联显著减弱(风险比 1.29,置信区间,0.99-1.68)。
老年心肌梗死患者在表现、治疗和结局方面存在很大差异。移动障碍是脆弱的标志,它改变了高龄与治疗以及结局之间的关联。