Miller Yvette D, Armanasco Ashleigh A, McCosker Laura, Thompson Rachel
Queensland University of Technology, Institute of Health & Biomedical Innovation, School of Public Health & Social Work, Kelvin Grove, Brisbane, QLD, 4059, Australia.
School of Public Health, Faculty of Medicine and Health, The University of Sydney, Camperdown, NSW, 2006, Australia.
BMC Pregnancy Childbirth. 2020 Aug 17;20(1):469. doi: 10.1186/s12884-020-03149-7.
There is no available evidence for the prevalence of early labour admission to hospital or its association with rates of intervention and clinical outcomes in Australia. The objectives of this study were to: estimate the prevalence of early labour admission in one hospital in Australia; compare rates of clinical intervention, length of hospital stay and clinical outcomes for women admitted in early (< 4 cm cervical dilatation) or active (≥4 cm) labour; and determine the impact of recent recommendations to define early labour as < 5 cm on the findings.
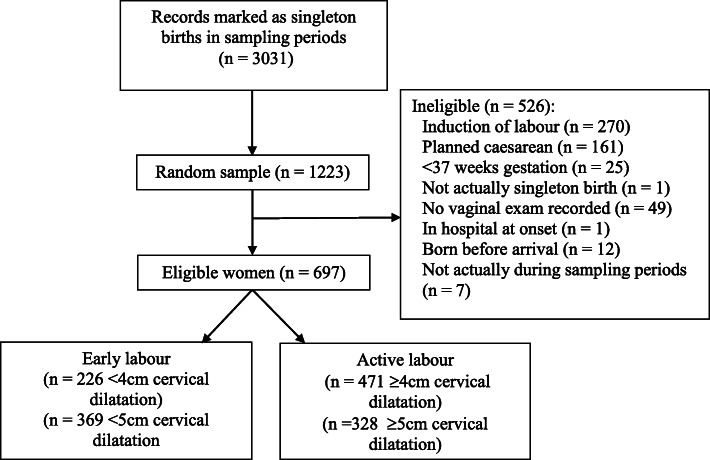
We conducted a retrospective cohort study using medical record data from a random sample of 1223 women from live singleton births recorded between July 2013 and December 2015. Analyses included women who had spontaneous onset of labour at ≥37 weeks gestation whilst not a hospital inpatient, who had not scheduled a caesarean section before labour onset or delivered prior to hospital admission. Associations between timing of hospital admission in labour and clinical intervention, outcomes and hospital stay were assessed using logistic regression.
Between 32.4% (< 4 cm) and 52.9% (< 5 cm) of eligible women (N = 697) were admitted to hospital in early labour. After adjustment for potential confounders, women admitted in early labour (< 4 cm) were more likely to have their labour augmented by oxytocin (AOR = 3.57, 95% CI 2.39-5.34), an epidural (AOR = 2.27, 95% CI 1.51-3.41), a caesarean birth (AOR = 3.50, 95% CI 2.10-5.83), more vaginal examinations (AOR = 1.73, 95% CI = 1.53-1.95), and their baby admitted to special care nursery (AOR = 1.54, 95% CI = 1.01-2.35). Defining early labour as < 5 cm cervical dilatation produced additional significant associations with artificial rupture of membranes (AOR = 1.41, 95% CI = 1.02-1.95), assisted vaginal birth (AOR = 1.96, 95% CI = 1.12-3.41) neonatal resuscitation (AOR = 1.73, 95% CI = 1.01-2.99) and longer maternal hospital stay (AOR = 1.21, 95% CI = 1.04-1.40).
Findings provide preliminary evidence that a notable proportion of labouring women are admitted in early labour and are more likely to experience several medical procedures, neonatal resuscitation and admission to special care nursery, and longer hospital stay.
在澳大利亚,尚无关于早产入院的患病率及其与干预率和临床结局之间关联的可用证据。本研究的目的是:估计澳大利亚一家医院早产入院的患病率;比较早产(宫颈扩张<4cm)或活跃期(≥4cm)入院的女性的临床干预率、住院时间和临床结局;并确定将早产定义为<5cm的最新建议对研究结果的影响。
我们进行了一项回顾性队列研究,使用了2013年7月至2015年12月期间记录的1223名单胎活产女性的随机样本的病历数据。分析包括妊娠≥37周自然发动分娩且非住院患者、分娩发动前未计划剖宫产或入院前未分娩的女性。使用逻辑回归评估分娩时入院时间与临床干预、结局和住院时间之间的关联。
符合条件的女性(N = 697)中,32.4%(<4cm)至52.9%(<5cm)在早产时入院。在调整潜在混杂因素后,早产(<4cm)入院的女性更有可能接受缩宫素引产(调整后比值比[AOR]=3.57,95%置信区间[CI]2.39 - 5.34)、硬膜外麻醉(AOR = 2.27,95%CI 1.51 - 3.41)、剖宫产(AOR = 3.50,95%CI 2.10 - 5.83)、更多的阴道检查(AOR = 1.73,95%CI = 1.53 - 1.95),以及她们的婴儿入住特殊护理病房(AOR = 1.54,95%CI = 1.01 - 2.35)。将早产定义为宫颈扩张<5cm会产生与人工破膜(AOR = 1.41,95%CI = 1.02 - 1.95)、阴道助产(AOR = 1.96,95%CI = 1.12 - 3.41)、新生儿复苏(AOR = 1.73,95%CI = 1.01 - 2.99)和产妇住院时间延长(AOR = 1.21,95%CI = 1.04 - 1.40)的额外显著关联。
研究结果提供了初步证据,表明相当比例的分娩女性在早产时入院,并且更有可能经历多种医疗程序、新生儿复苏和入住特殊护理病房,以及住院时间延长。