Sauthier Michaël S, Jouvet Philippe A, Newhams Margaret M, Randolph Adrienne G
Departments of Pediatrics, Sainte-Justine Hospital, Montreal, QC, Canada.
Department of Anesthesiology, Critical Care and Pain Medicine, Boston Children's Hospital, Boston, MA.
Crit Care Explor. 2020 Aug 6;2(8):e0175. doi: 10.1097/CCE.0000000000000175. eCollection 2020 Aug.
Influenza virus is a major cause of acute hypoxemic respiratory failure. Early identification of patients who will suffer severe complications can help stratify patients for clinical trials and plan for resource use in case of pandemic.
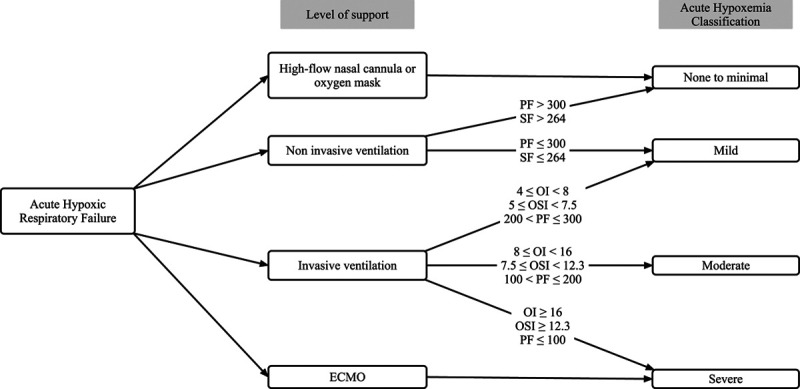
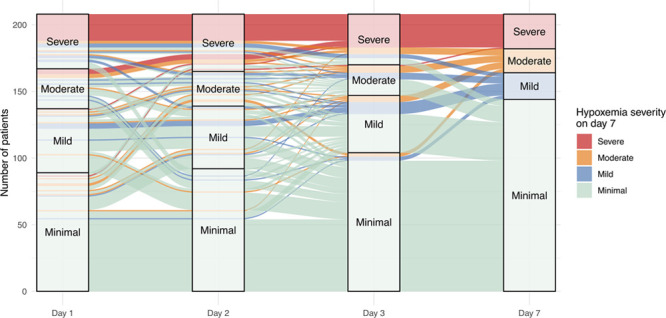
We aimed to identify which clinical variables best predict prolonged acute hypoxemic respiratory failure in influenza-infected critically ill children. Acute hypoxemic respiratory failure was defined using hypoxemia cutoffs from international consensus definitions of acute respiratory distress syndrome in patients with ventilatory support. Prolonged acute hypoxemic respiratory failure was defined by acute hypoxemic respiratory failure criteria still present at PICU day 7.
In this prospective multicenter study across 34 PICUs from November 2009 to April 2018, we included children (< 18 yr) without comorbid risk factors for severe disease.
We used a Monte Carlo cross validation method with random train-test splits at a 70-30% proportion per model.
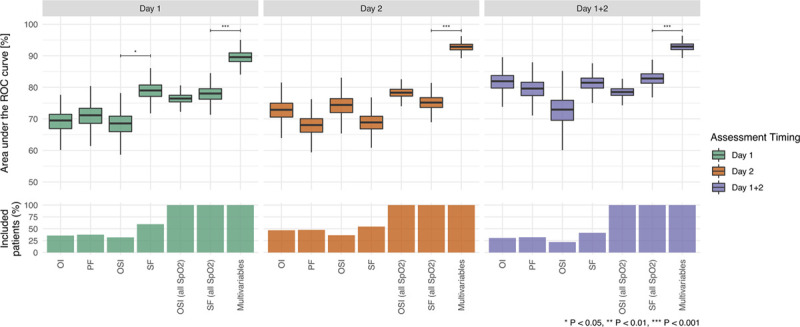
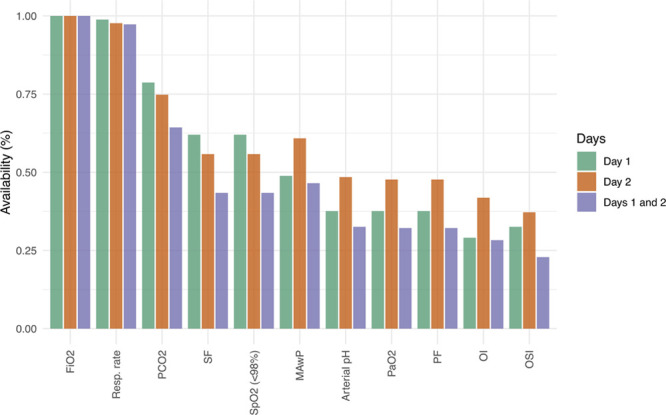
Using clinical data at admission (day 1) and closest to 8 am on PICU day 2, we calculated the area under the receiver operating characteristic curve using random forests machine learning algorithms and logistic regression.
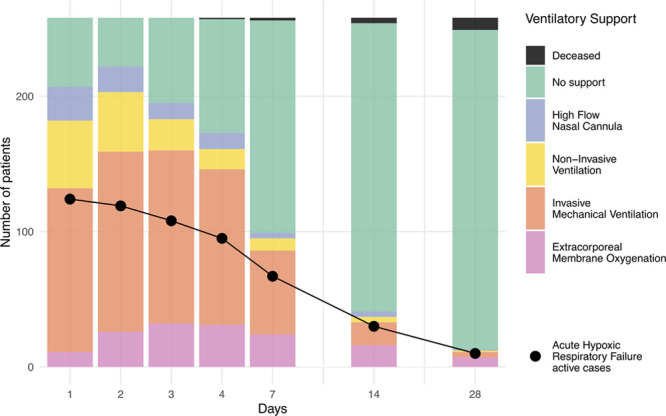
We included 258 children (median age = 6.5 yr) and 11 (4.2%) died. By day 2, 65% ( = 165) had acute hypoxemic respiratory failure dropping to 26% ( = 67) with prolonged acute hypoxemic respiratory failure by day 7. Those with prolonged acute hypoxemic respiratory failure had a longer ICU stay (16.5 vs 4.0 d; < 0.001) and higher mortality (13.4% vs 1.0%). A multivariable model using random forests with 10 admission and eight day 2 variables performed best (0.93 area under the receiver operating characteristic curve; 95 CI%: 0.90-0.95) where respiratory rate, Fio, and pH on day 2 were the most important factors.
In this prospective multicentric study, most children with influenza virus-related respiratory failure with prolonged acute hypoxemic respiratory failure can be identified early in their hospital course applying machine learning onto routine clinical data. Further validation is needed prior to bedside implementation.
流感病毒是急性低氧性呼吸衰竭的主要病因。早期识别可能出现严重并发症的患者有助于对患者进行分层以便开展临床试验,并在大流行情况下规划资源使用。
我们旨在确定哪些临床变量最能预测流感感染的危重症儿童出现持续性急性低氧性呼吸衰竭。急性低氧性呼吸衰竭采用通气支持患者急性呼吸窘迫综合征国际共识定义中的低氧血症临界值来定义。持续性急性低氧性呼吸衰竭定义为重症监护病房(PICU)第7天时仍符合急性低氧性呼吸衰竭标准。
在这项2009年11月至2018年4月期间横跨34个PICU的前瞻性多中心研究中,我们纳入了无严重疾病合并危险因素的儿童(<18岁)。
我们使用蒙特卡洛交叉验证方法,每个模型按70 - 30%的比例进行随机训练 - 测试划分。
利用入院时(第1天)和PICU第2天最接近上午8点的临床数据,我们使用随机森林机器学习算法和逻辑回归计算受试者操作特征曲线下面积。
我们纳入了258名儿童(中位年龄 = 6.5岁),11名(4.2%)死亡。到第2天,65%(n = 165)出现急性低氧性呼吸衰竭,到第7天持续性急性低氧性呼吸衰竭的比例降至26%(n = 67)。出现持续性急性低氧性呼吸衰竭的患者在ICU的住院时间更长(16.5天对4.0天;P < 0.001),死亡率更高(13.4%对1.0%)。使用随机森林的多变量模型,纳入10个入院变量和8个第2天变量时表现最佳(受试者操作特征曲线下面积为0.93;95%置信区间:0.90 - 0.95),其中第2天的呼吸频率、吸入氧分数和pH值是最重要的因素。
在这项前瞻性多中心研究中,通过将机器学习应用于常规临床数据,大多数患有流感病毒相关呼吸衰竭且出现持续性急性低氧性呼吸衰竭的儿童在其住院过程中可被早期识别。在床边实施之前还需要进一步验证。