Institut Pierre Louis d'Épidémiologie et de Santé Publique, Sorbonne Université, INSERM, Paris, France.
Virology Department, Pasteur Centre of Cameroon, Yaoundé, Cameroon.
PLoS One. 2020 Aug 24;15(8):e0238035. doi: 10.1371/journal.pone.0238035. eCollection 2020.
Whereas 72% of hepatitis C virus (HCV)-infected people worldwide live in low- and middle-income countries (LMICs), only 6% of them have been diagnosed. Innovative technologies for HCV diagnosis provide opportunities for developing testing strategies more adapted to resource-constrained settings. However, studies about their economic feasibility in LMICs are lacking.
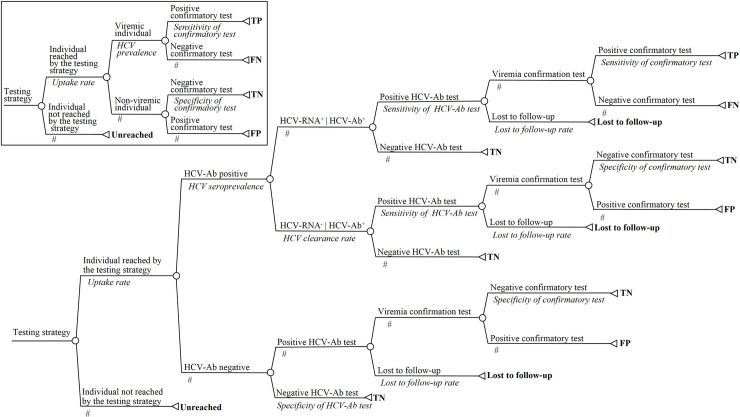
Adopting a health sector perspective in Cameroon, Cote-d'Ivoire, and Senegal, a decision tree model was developed to compare 12 testing strategies with the following characteristics: a one-step or two-step testing sequence, HCV-RNA or HCV core antigen as confirmative biomarker, laboratory or point-of-care (POC) tests, and venous blood samples or dried blood spots (DBS). Outcomes measures were the number of true positives (TPs), cost per screened individual, incremental cost-effectiveness ratios, and nationwide budget. Corresponding time horizon was immediate, and outcomes were accordingly not discounted. Detailed sensitivity analyses were conducted.
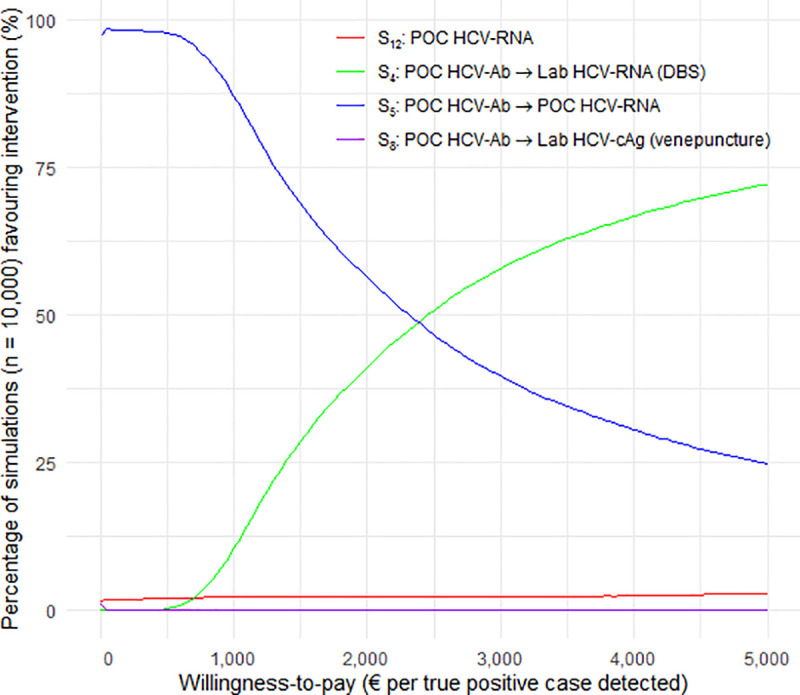
In the base-case, a two-step POC-based strategy including anti-HCV antibody (HCV-Ab) and HCV-RNA testing had the lowest cost, €8.18 per screened individual. Assuming a lost-to-follow-up rate after screening > 1.9%, a DBS-based laboratory HCV-RNA after HCV-Ab POC testing was the single un-dominated strategy, requiring an additional cost of €3653.56 per additional TP detected. Both strategies would require 8-25% of the annual public health expenditure of the study countries for diagnosing 30% of HCV-infected individuals. Assuming a seroprevalence > 46.9% or a cost of POC HCV-RNA < €7.32, a one-step strategy based on POC HCV-RNA dominated the two-step POC-based strategy but resulted in many more false-positive cases.
POC HCV-Ab followed by either POC- or DBS-based HCV-RNA testing would be the most cost-effective strategies in the study countries. Without a substantial increase in funding for health or a dramatic decrease in assay prices, HCV testing would constitute an economic barrier to the implementation of HCV elimination programs in LMICs.
全球范围内,72%的丙型肝炎病毒(HCV)感染者生活在中低收入国家(LMICs),但仅有 6%的人得到了诊断。HCV 诊断的创新技术为开发更适合资源有限环境的检测策略提供了机会。然而,关于这些技术在 LMICs 中经济可行性的研究尚不多见。
在喀麦隆、科特迪瓦和塞内加尔,采用卫生部门视角,建立决策树模型,比较了 12 种检测策略,这些策略具有以下特点:一步或两步检测序列、HCV-RNA 或 HCV 核心抗原作为确证性生物标志物、实验室或即时检测(POC)检测以及静脉血样或干血斑(DBS)。结果指标是真阳性(TPs)数量、每个筛查个体的成本、增量成本效益比和全国预算。相应的时间范围是即时的,因此结果没有贴现。进行了详细的敏感性分析。
在基础案例中,基于 POC 的两步策略,包括抗 HCV 抗体(HCV-Ab)和 HCV-RNA 检测,成本最低,每个筛查个体 8.18 欧元。假设筛查后失访率>1.9%,基于 DBS 的实验室 HCV-RNA 检测是唯一的非主导策略,检测到额外的 1 个 TP 需要额外增加 3653.56 欧元。这两种策略都需要研究国家年度公共卫生支出的 8-25%,以诊断 30%的 HCV 感染者。假设血清流行率>46.9%或 POC HCV-RNA 成本<8.32 欧元,基于 POC HCV-RNA 的一步策略优于两步基于 POC 的策略,但会导致更多的假阳性病例。
在研究国家中,基于 POC 的 HCV-Ab 检测,然后是基于 POC 或 DBS 的 HCV-RNA 检测,将是最具成本效益的策略。如果没有对卫生保健的大量资金投入增加,或者检测价格没有大幅下降,HCV 检测将成为在 LMICs 中实施 HCV 消除计划的经济障碍。