Institute of Medical Microbiology, University of Zurich, 8006 Zurich, Switzerland.
Int J Mol Sci. 2020 Aug 25;21(17):6133. doi: 10.3390/ijms21176133.
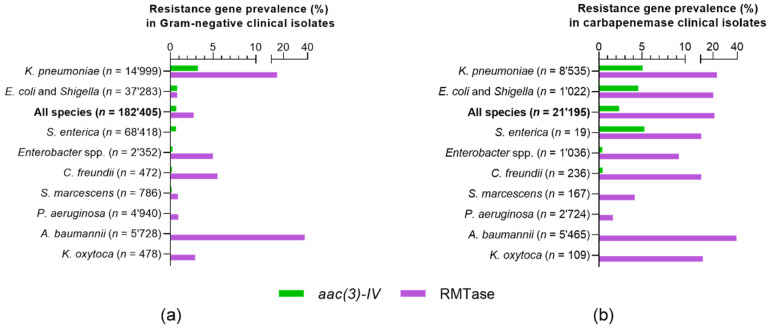
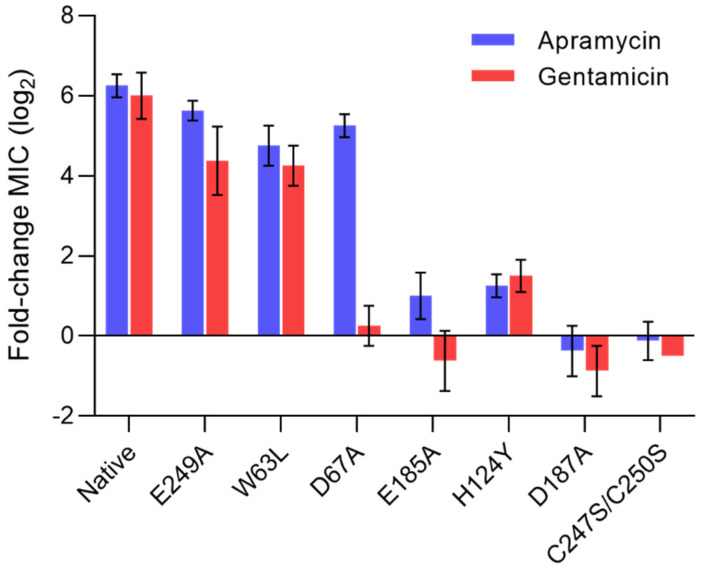
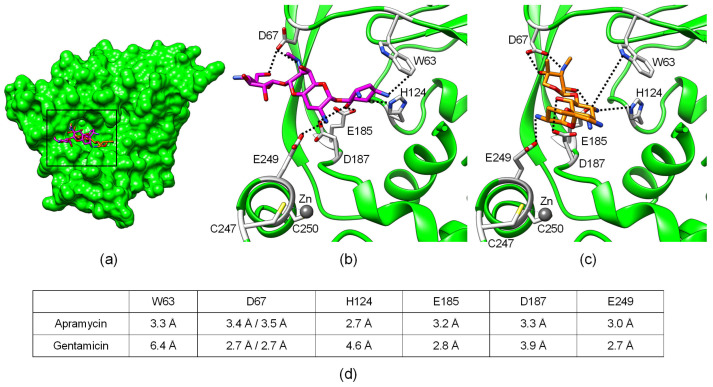
Aminoglycoside antibiotics are powerful bactericidal therapeutics that are often used in the treatment of critical Gram-negative systemic infections. The emergence and global spread of antibiotic resistance, however, has compromised the clinical utility of aminoglycosides to an extent similar to that found for all other antibiotic-drug classes. Apramycin, a drug candidate currently in clinical development, was suggested as a next-generation aminoglycoside antibiotic with minimal cross-resistance to all other standard-of-care aminoglycosides. Here, we analyzed 591,140 pathogen genomes deposited in the NCBI National Database of Antibiotic Resistant Organisms (NDARO) for annotations of apramycin-resistance genes, and compared them to the genotypic prevalence of carbapenem resistance and 16S-rRNA methyltransferase (RMTase) genes. The 3--acetyltransferase gene was found to be the only apramycin-resistance gene of clinical relevance, at an average prevalence of 0.7%, which was four-fold lower than that of RMTase genes. In the important subpopulation of carbapenemase-positive isolates, was nine-fold less prevalent than RMTase genes. The phenotypic profiling of selected clinical isolates and recombinant strains expressing the gene confirmed resistance to not only apramycin, but also gentamicin, tobramycin, and paromomycin. Probing the structure-activity relationship of such substrate promiscuity by site-directed mutagenesis of the aminoglycoside-binding pocket in the acetyltransferase AAC(3)-IV revealed the molecular contacts to His124, Glu185, and Asp187 to be equally critical in binding to apramycin and gentamicin, whereas Asp67 was found to be a discriminating contact. Our findings suggest that aminoglycoside cross-resistance to apramycin in clinical isolates is limited to the substrate promiscuity of a single gene, rendering apramycin best-in-class for the coverage of carbapenem- and aminoglycoside-resistant bacterial infections.
氨基糖苷类抗生素是一种强大的杀菌治疗药物,常用于治疗严重的革兰氏阴性全身感染。然而,抗生素耐药性的出现和全球传播已经在一定程度上削弱了氨基糖苷类药物的临床实用性,这与所有其他抗生素药物类别相同。阿米卡星是一种目前正在临床开发的药物候选物,被认为是一种具有最小交叉耐药性的新一代氨基糖苷类抗生素,对所有其他标准护理氨基糖苷类药物都具有最小的交叉耐药性。在这里,我们分析了 NCBI 国家抗生素耐药生物体数据库 (NDARO) 中 591140 个病原体基因组,以确定阿米卡星耐药基因的注释,并将其与碳青霉烯类耐药基因和 16S-rRNA 甲基转移酶 (RMTase) 基因的基因型流行率进行比较。我们发现 3--乙酰转移酶基因是唯一具有临床相关性的阿米卡星耐药基因,其平均流行率为 0.7%,是 RMTase 基因的四倍。在重要的碳青霉烯酶阳性分离株亚群中,的流行率比 RMTase 基因低九倍。对选定临床分离株和表达基因的重组株的表型分析证实,不仅对阿米卡星,而且对庆大霉素、妥布霉素和巴龙霉素均有耐药性。通过对乙酰转移酶 AAC(3)-IV 的氨基糖苷结合口袋进行定点突变来探测这种底物混杂的结构-活性关系,揭示了与 His124、Glu185 和 Asp187 的分子接触在结合阿米卡星和庆大霉素方面同样重要,而 Asp67 则被发现是一个有区别的接触点。我们的研究结果表明,临床分离株中氨基糖苷类抗生素对阿米卡星的交叉耐药性仅限于单个基因的底物混杂性,使阿米卡星成为治疗碳青霉烯类和氨基糖苷类耐药细菌感染的最佳选择。