Laboratorio de Neuropatología Molecular, Instituto de Biología Celular y Neurociencia "Prof. E. De Robertis," Facultad de Medicina, UBA-CONICET, Universidad de Buenos Aires, Ciudad de Buenos Aires, Argentina.
ASN Neuro. 2020 Jan-Dec;12:1759091420954960. doi: 10.1177/1759091420954960.
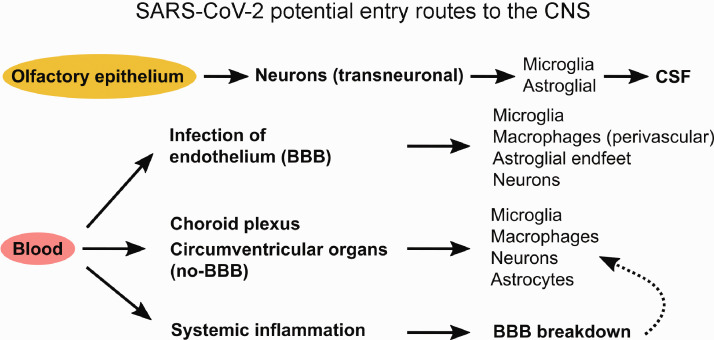
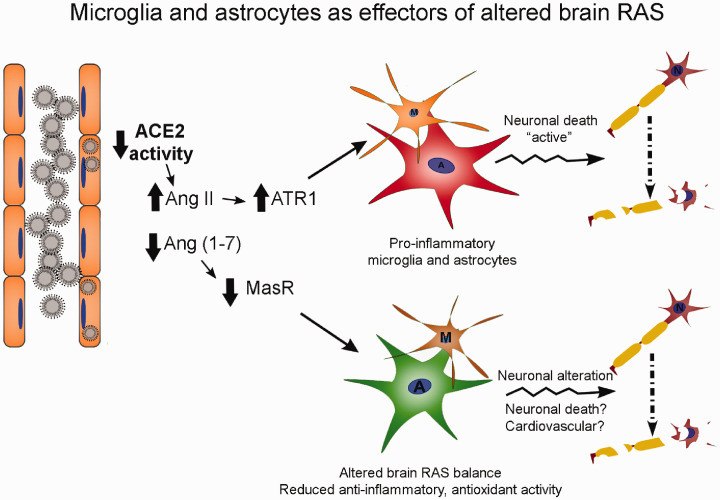
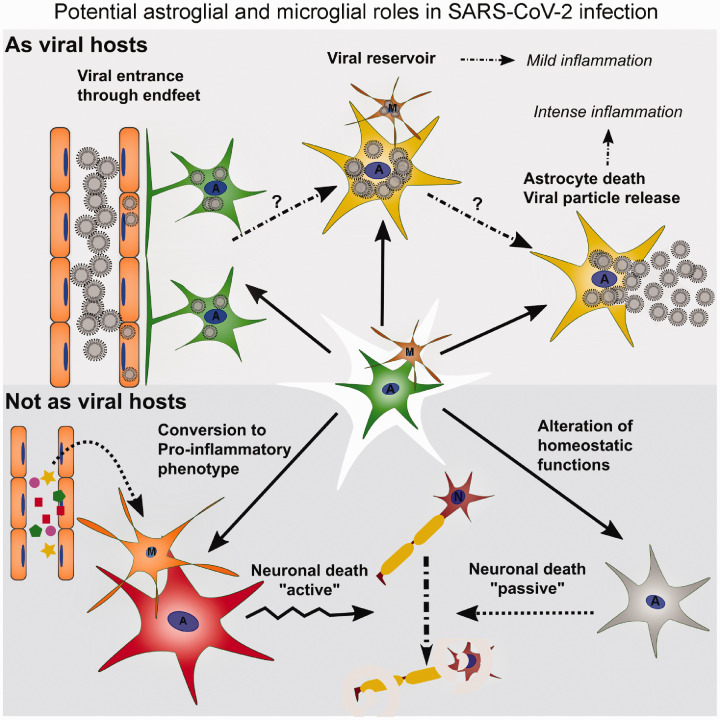
With confirmed coronavirus disease 2019 (COVID-19) cases surpassing the 18 million mark around the globe, there is an imperative need to gain comprehensive understanding of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Although the main clinical manifestations of COVID-19 are associated with respiratory or intestinal symptoms, reports of neurological signs and symptoms are increasing. The etiology of these neurological manifestations remains obscure, and probably involves several direct pathways, not excluding the direct entry of the virus to the central nervous system (CNS) through the olfactory epithelium, circumventricular organs, or disrupted blood-brain barrier. Furthermore, neuroinflammation might occur in response to the strong systemic cytokine storm described for COVID-19, or due to dysregulation of the CNS rennin-angiotensin system. Descriptions of neurological manifestations in patients in the previous coronavirus (CoV) outbreaks have been numerous for the SARS-CoV and lesser for Middle East respiratory syndrome coronavirus (MERS-CoV). Strong evidence from patients and experimental models suggests that some human variants of CoV have the ability to reach the CNS and that neurons, astrocytes, and/or microglia can be target cells for CoV. A growing body of evidence shows that astrocytes and microglia have a major role in neuroinflammation, responding to local CNS inflammation and/or to disbalanced peripheral inflammation. This is another potential mechanism for SARS-CoV-2 damage to the CNS. In this comprehensive review, we will summarize the known neurological manifestations of SARS-CoV-2, SARS-CoV and MERS-CoV; explore the potential role for astrocytes and microglia in the infection and neuroinflammation; and compare them with the previously described human and animal CoV that showed neurotropism to propose possible underlying mechanisms.
随着全球确诊的 2019 冠状病毒病 (COVID-19) 病例超过 1800 万例,人们迫切需要全面了解严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2)。尽管 COVID-19 的主要临床症状与呼吸道或肠道症状有关,但越来越多的报告显示存在神经系统症状和体征。这些神经系统表现的病因尚不清楚,可能涉及几种直接途径,不能排除病毒通过嗅上皮、室周器官或血脑屏障破坏直接进入中枢神经系统 (CNS)。此外,神经炎症可能是由于 COVID-19 中描述的强烈全身细胞因子风暴,或由于中枢神经系统肾素-血管紧张素系统失调引起的。以前冠状病毒 (CoV) 爆发中患者的神经系统表现已有大量描述,SARS-CoV 较多,而中东呼吸综合征冠状病毒 (MERS-CoV) 较少。来自患者和实验模型的强有力证据表明,一些人类 CoV 变体有能力到达中枢神经系统,神经元、星形胶质细胞和/或小胶质细胞可能是 CoV 的靶细胞。越来越多的证据表明,星形胶质细胞和小胶质细胞在神经炎症中起主要作用,它们对局部中枢神经系统炎症和/或失衡的外周炎症作出反应。这是 SARS-CoV-2 对中枢神经系统造成损害的另一个潜在机制。在这篇综合综述中,我们将总结 SARS-CoV-2、SARS-CoV 和 MERS-CoV 的已知神经系统表现;探讨星形胶质细胞和小胶质细胞在感染和神经炎症中的潜在作用;并将它们与以前描述的具有嗜神经特性的人类和动物 CoV 进行比较,提出可能的潜在机制。