Departments of Imaging, Medicine, Smidt Heart Institute and Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, 116 N Robertson Blvd, Los Angeles, CA, 90048, USA.
Department of Cardiac Sciences, University of Calgary, Calgary, AB, Canada.
Eur Radiol. 2021 Mar;31(3):1227-1235. doi: 10.1007/s00330-020-07142-8. Epub 2020 Sep 3.
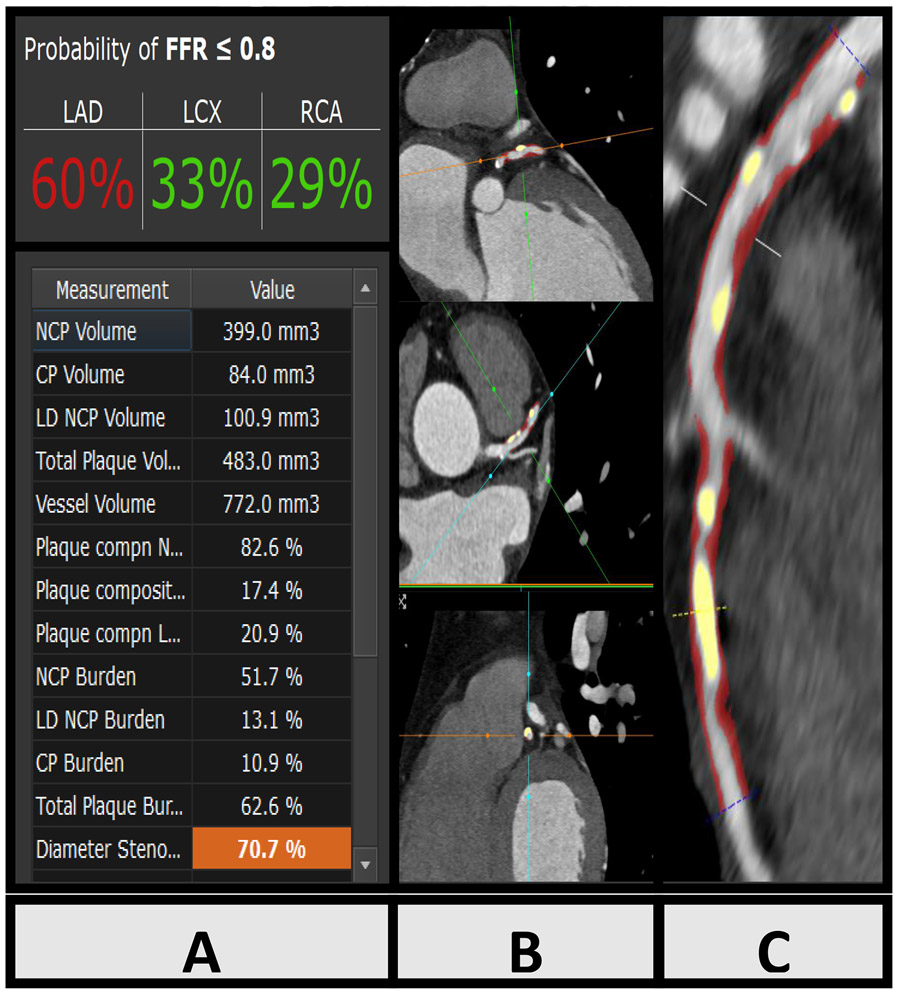
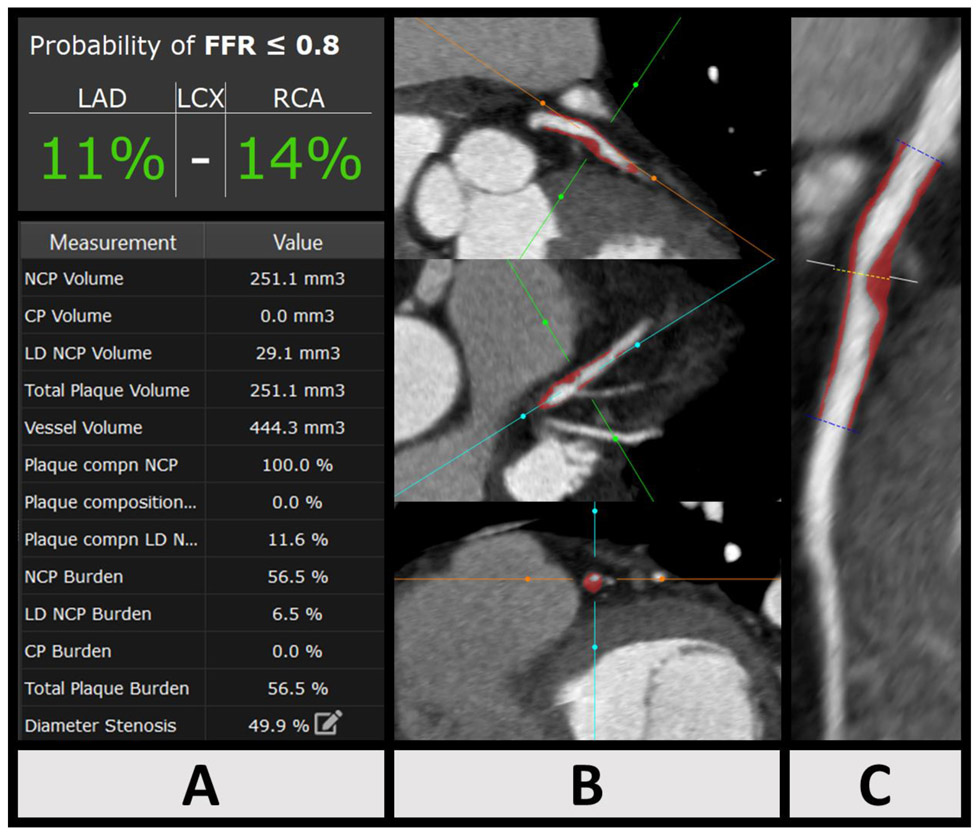
The machine learning ischemia risk score (ML-IRS) is a machine learning-based algorithm designed to identify hemodynamically significant coronary disease using quantitative coronary computed tomography angiography (CCTA). The purpose of this study was to examine whether the ML-IRS can predict revascularization in patients referred for invasive coronary angiography (ICA) after CCTA.
This study was a post hoc analysis of a prospective dual-center registry of sequential patients undergoing CCTA followed by ICA within 3 months, referred from inpatient, outpatient, and emergency department settings (n = 352, age 63 ± 10 years, 68% male). The primary outcome was revascularization by either percutaneous coronary revascularization or coronary artery bypass grafting. Blinded readers performed semi-automated quantitative coronary plaque analysis. The ML-IRS was automatically computed. Relationships between clinical risk factors, coronary plaque features, and ML-IRS with revascularization were examined.
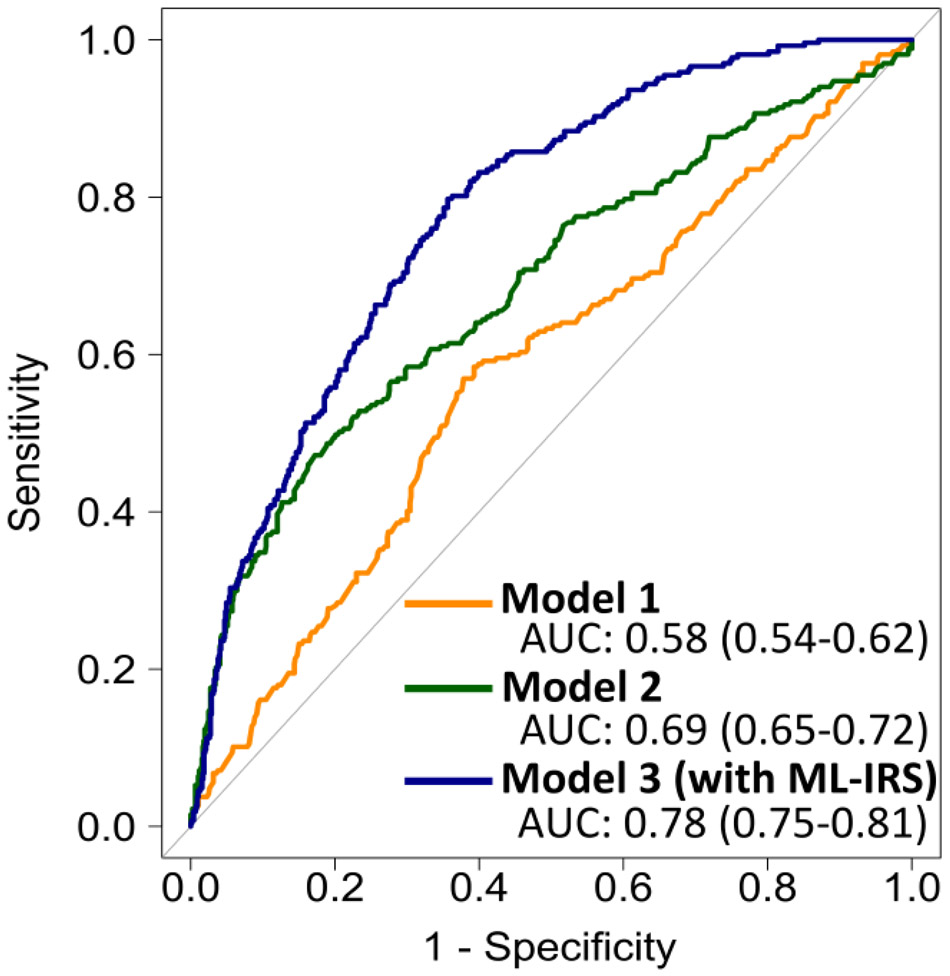
The study cohort consisted of 352 subjects with 1056 analyzable vessels. The ML-IRS ranged between 0 and 81% with a median of 18.7% (6.4-34.8). Revascularization was performed in 26% of vessels. Vessels receiving revascularization had higher ML-IRS (33.6% (21.1-55.0) versus 13.0% (4.5-29.1), p < 0.0001), as well as higher contrast density difference, and total, non-calcified, calcified, and low-density plaque burden. ML-IRS, when added to a traditional risk model based on clinical data and stenosis to predict revascularization, resulted in increased area under the curve from 0.69 (95% CI: 0.65-0.72) to 0.78 (95% CI: 0.75-0.81) (p < 0.0001), with an overall continuous net reclassification improvement of 0.636 (95% CI: 0.503-0.769; p < 0.0001).
ML-IRS from quantitative coronary CT angiography improved the prediction of future revascularization and can potentially identify patients likely to receive revascularization if referred to cardiac catheterization.
• Machine learning ischemia risk from quantitative coronary CT angiography was significantly higher in patients who received revascularization versus those who did not receive revascularization. • The machine learning ischemia risk score was significantly higher in patients with invasive fractional flow ≤ 0.8 versus those with > 0.8. • The machine learning ischemia risk score improved the prediction of future revascularization significantly when added to a standard prediction model including stenosis.
机器学习缺血风险评分(ML-IRS)是一种基于机器学习的算法,旨在使用定量冠状动脉计算机断层血管造影术(CCTA)识别血流动力学意义重大的冠状动脉疾病。本研究的目的是检验 ML-IRS 是否可以预测 CCTA 后行有创冠状动脉造影(ICA)的患者进行血运重建的情况。
这是一项对前瞻性、双中心连续患者的回顾性分析,这些患者在 CCTA 后 3 个月内行 ICA,这些患者来自住院、门诊和急诊环境(n=352,年龄 63±10 岁,68%为男性)。主要结局是通过经皮冠状动脉血运重建或冠状动脉旁路移植术进行血运重建。盲法读者进行半自动定量冠状动脉斑块分析。自动计算 ML-IRS。检查临床危险因素、冠状动脉斑块特征和 ML-IRS 与血运重建之间的关系。
研究队列包括 352 例患者,共 1056 个可分析血管。ML-IRS 范围为 0%至 81%,中位数为 18.7%(6.4-34.8)。26%的血管接受了血运重建。接受血运重建的血管 ML-IRS 更高(33.6%(21.1-55.0)比 13.0%(4.5-29.1),p<0.0001),以及更高的对比密度差异、总、非钙化、钙化和低密度斑块负担。ML-IRS 与基于临床数据和狭窄的传统风险模型相结合,用于预测血运重建,曲线下面积从 0.69(95%CI:0.65-0.72)增加到 0.78(95%CI:0.75-0.81)(p<0.0001),总体连续净重新分类改善率为 0.636(95%CI:0.503-0.769;p<0.0001)。
来自定量冠状动脉 CT 血管造影的机器学习缺血风险评分提高了对未来血运重建的预测能力,如果将其转诊至心导管检查,可能有助于识别可能需要血运重建的患者。
与未接受血运重建的患者相比,接受血运重建的患者的定量冠状动脉 CT 血管造影术的机器学习缺血风险评分显著更高。
与狭窄程度>0.8 的患者相比,狭窄程度≤0.8 的患者的机器学习缺血风险评分显著更高。
当 ML-IRS 与包括狭窄程度的标准预测模型结合使用时,其对未来血运重建的预测显著提高。