Lynch Shannon M, Wiese Daniel, Ortiz Angel, Sorice Kristen A, Nguyen Minhhuyen, González Evelyn T, Henry Kevin A
Cancer Prevention and Control, Fox Chase Cancer Center, Philadelphia, PA, USA.
Geography and Urban Studies, Temple University, Philadelphia, PA, USA.
SSM Popul Health. 2020 Aug 7;12:100640. doi: 10.1016/j.ssmph.2020.100640. eCollection 2020 Dec.
Liver cancer (LC) continues to rise, partially due to limited resources for prevention. To test the precision public health (PPH) hypothesis that fewer areas in need of LC prevention could be identified by combining existing surveillance data, we compared the sensitivity/specificity of standard recommendations to target geographic areas using U.S. Census demographic data only (percent (%) Hispanic, Black, and those born 1950-1959) to an alternative approach that couples additional geospatial data, including neighborhood socioeconomic status (nSES), with LC disease statistics.
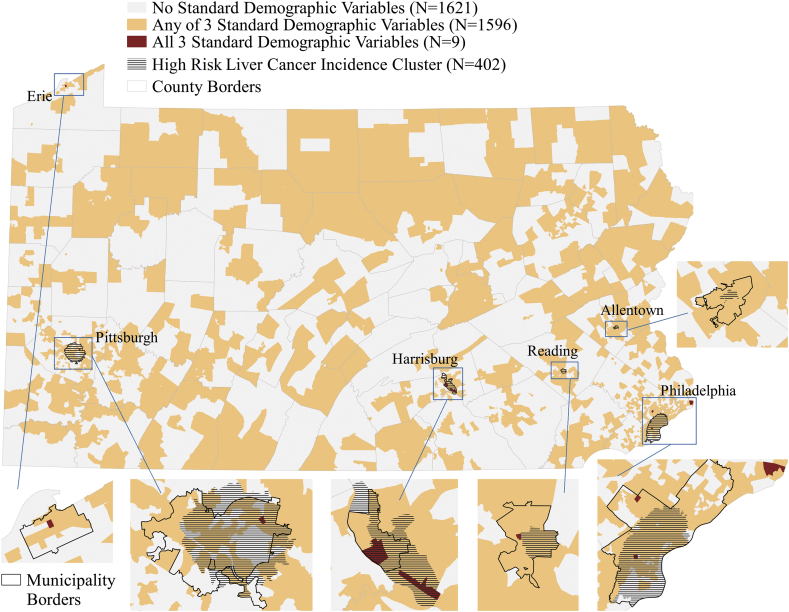
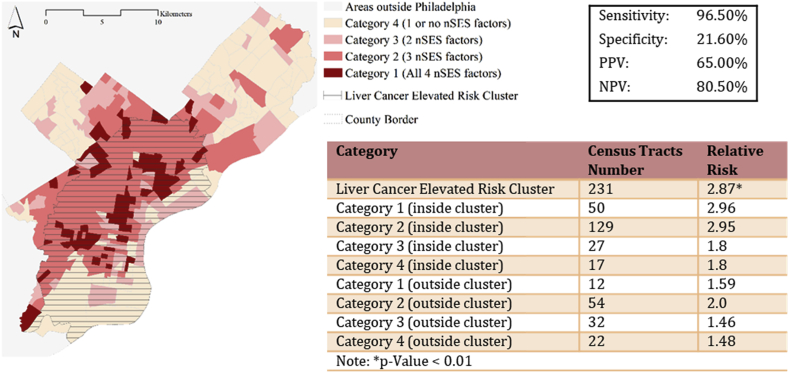
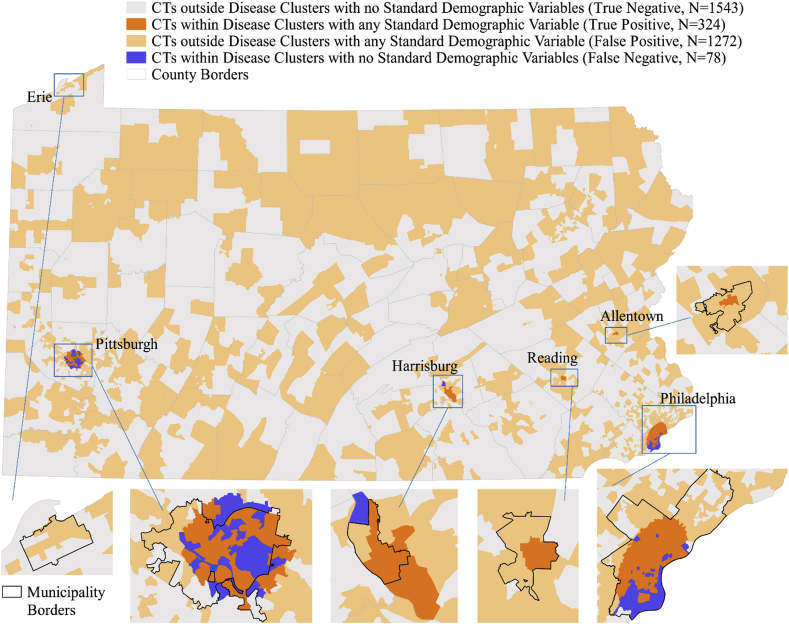
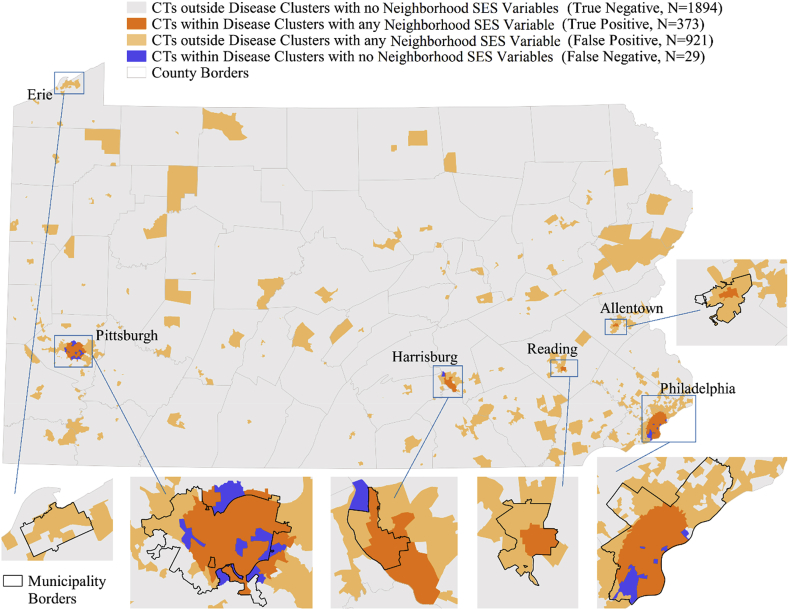
Pennsylvania Cancer Registry data from 2007-2014 were linked to 2010 U.S. Census data at the Census tract (CT) level. CTs in the top 80th percentile for 3 standard demographic variables, %Hispanic, %Black, %born 1950-1959, were identified. Spatial scan statistics (SatScan) identified CTs with significantly elevated incident LC rates (p-value<0.05), adjusting for age, gender, diagnosis year. Sensitivity, specificity, and positive predictive value (PPV) of a CT being located in an elevated risk cluster and/or testing positive/negative for at least one standard variable were calculated. nSES variables (deprivation, stability, segregation) significantly associated with LC in regression models (p < 0.05) were systematically evaluated for improvements in sensitivity/specificity.
9,460 LC cases were diagnosed across 3,217 CTs. 1,596 CTs were positive for at least one of 3 standard variables. 5 significant elevated risk clusters (CTs = 402) were identified. 324 CTs were positive for a high risk cluster AND standard variable (sensitivity = 92%; specificity = 37%; PPV = 17.4%). Incorporation of 3 new nSES variables with one standard variable (%Black) further improved sensitivity (93%), specificity (62.9%), and PPV (26.3%).
We introduce a quantitative assessment of PPH by applying established sensitivity/specificity assessments to geospatial data. Coupling existing disease cluster and nSES data can more precisely identify intervention targets with a liver cancer burden than standard demographic variables. Thus, this approach may inform prioritization of limited resources for liver cancer prevention.
肝癌(LC)的发病率持续上升,部分原因是预防资源有限。为了验证精准公共卫生(PPH)假说,即通过整合现有监测数据能够识别出更少的需要进行肝癌预防的地区,我们比较了仅使用美国人口普查人口统计数据(西班牙裔、黑人以及1950 - 1959年出生人口的百分比)来确定肝癌预防目标地理区域的标准建议的敏感性/特异性,与一种将包括邻里社会经济地位(nSES)在内的额外地理空间数据与肝癌疾病统计数据相结合的替代方法的敏感性/特异性。
将2007 - 2014年宾夕法尼亚癌症登记处的数据与2010年美国人口普查数据在普查区(CT)层面进行关联。确定了在3个标准人口统计变量(西班牙裔百分比、黑人百分比、1950 - 1959年出生人口百分比)处于第80百分位以上的普查区。空间扫描统计(SatScan)识别出肝癌发病率显著升高的普查区(p值<0.05),并对年龄、性别、诊断年份进行了调整。计算了普查区位于高风险集群中和/或至少一个标准变量检测呈阳性/阴性的敏感性、特异性和阳性预测值(PPV)。对回归模型中与肝癌显著相关(p < 0.05)的nSES变量(贫困、稳定性、隔离)进行系统评估,以确定其对敏感性/特异性的改善情况。
在3217个普查区共诊断出9460例肝癌病例。1596个普查区至少有一个标准变量呈阳性。识别出5个显著的高风险集群(普查区 = 402)。324个普查区高风险集群和标准变量均呈阳性(敏感性 = 92%;特异性 = 37%;PPV = 17.4%)。将3个新的nSES变量与一个标准变量(黑人百分比)相结合,进一步提高了敏感性(93%)、特异性(62.9%)和PPV(26.3%)。
我们通过将既定的敏感性/特异性评估应用于地理空间数据,对精准公共卫生进行了定量评估。与标准人口统计变量相比,将现有疾病集群数据和nSES数据相结合能够更精准地识别出承担肝癌负担的干预目标。因此,这种方法可为肝癌预防有限资源的优先排序提供参考。