Telethon Kids Institute, University of Western Australia, Nedlands, WA 6009, Australia.
School of Medicine, The University of Western Australia, Perth, WA 6009, Australia.
Int J Mol Sci. 2020 Sep 2;21(17):6372. doi: 10.3390/ijms21176372.
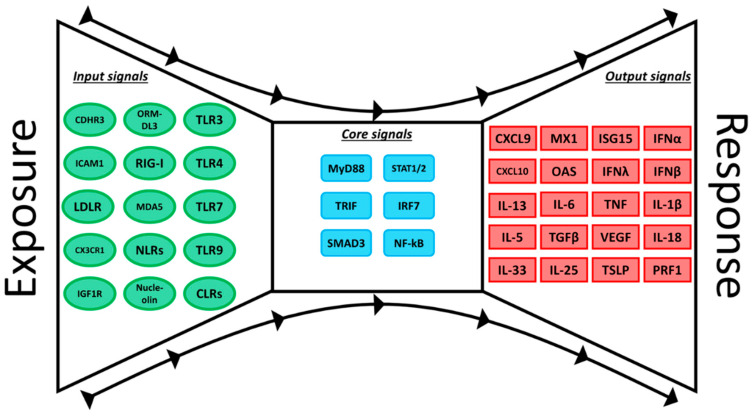
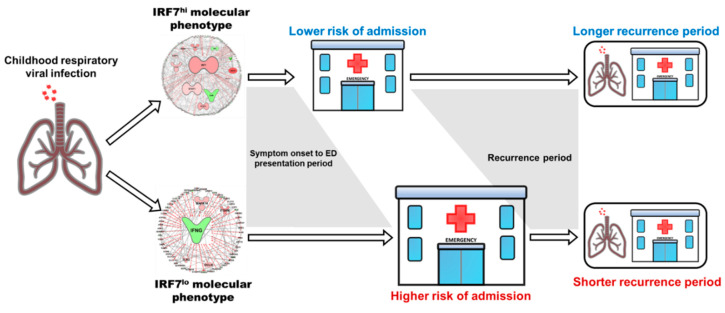
Human Respiratory Syncytial Virus and Human Rhinovirus are the most frequent cause of respiratory tract infections in infants and children and are major triggers of acute viral bronchiolitis, wheezing and asthma exacerbations. Here, we will discuss the application of the powerful tools of systems biology to decode the molecular mechanisms that determine risk for infection and subsequent asthma. An important conceptual advance is the understanding that the innate immune system is governed by a Bow-tie architecture, where diverse input signals converge onto a few core pathways (e.g., IRF7), which in turn generate diverse outputs that orchestrate effector and regulatory functions. Molecular profiling studies in children with severe exacerbations of asthma/wheeze have identified two major immunological phenotypes. The IRF7hi phenotype is characterised by robust upregulation of antiviral response networks, and the IRF7lo phenotype is characterised by upregulation of markers of TGFβ signalling and type 2 inflammation. Similar phenotypes have been identified in infants and children with severe viral bronchiolitis. Notably, genome-wide association studies supported by experimental validation have identified key pathways that increase susceptibility to HRV infection (ORMDL3 and CHDR3) and modulate TGFβ signalling (GSDMB, TGFBR1, and SMAD3). Moreover, functional deficiencies in the activation of type I and III interferon responses are already evident at birth in children at risk of developing febrile lower respiratory tract infections and persistent asthma/wheeze, suggesting that the trajectory to asthma begins at birth or in utero. Finally, exposure to microbes and their products reprograms innate immunity and provides protection from the development of allergies and asthma in children, and therefore microbial products are logical candidates for the primary prevention of asthma.
人呼吸道合胞病毒和人类鼻病毒是导致婴儿和儿童呼吸道感染的最常见原因,也是急性病毒性细支气管炎、喘息和哮喘恶化的主要诱因。在这里,我们将讨论系统生物学的强大工具在解码决定感染风险和随后哮喘的分子机制方面的应用。一个重要的概念性进展是认识到先天免疫系统受蝴蝶结结构控制,其中各种输入信号汇聚到少数核心途径(例如,IRF7),而这些途径又产生多样化的输出,从而协调效应器和调节功能。对哮喘/喘息严重恶化儿童的分子谱研究确定了两种主要的免疫学表型。IRF7hi 表型的特征是抗病毒反应网络的强烈上调,而 IRF7lo 表型的特征是 TGFβ 信号和 2 型炎症标志物的上调。在严重病毒性细支气管炎的婴儿和儿童中也发现了类似的表型。值得注意的是,全基因组关联研究得到实验验证的支持,确定了增加 HRV 感染易感性的关键途径(ORMDL3 和 CHDR3)和调节 TGFβ 信号(GSDMB、TGFBR1 和 SMAD3)的关键途径。此外,在有发生发热性下呼吸道感染和持续性哮喘/喘息风险的儿童中,出生时就已经存在 I 型和 III 型干扰素反应激活的功能缺陷,这表明哮喘的轨迹始于出生或宫内。最后,微生物及其产物的暴露重新编程先天免疫,并为儿童预防过敏和哮喘提供保护,因此微生物产物是预防哮喘的合理候选物。