Division of Cardiology, Pulmonology and Vascular Medicine, Heinrich Heine University, Moorenstr. 5, 40225, Düsseldorf, Germany.
CARID (Cardiovascular Research Institute Düsseldorf), Heinrich Heine University, Moorenstr. 5, 40225, Düsseldorf, Germany.
Heart Vessels. 2021 Feb;36(2):242-251. doi: 10.1007/s00380-020-01688-9. Epub 2020 Sep 7.
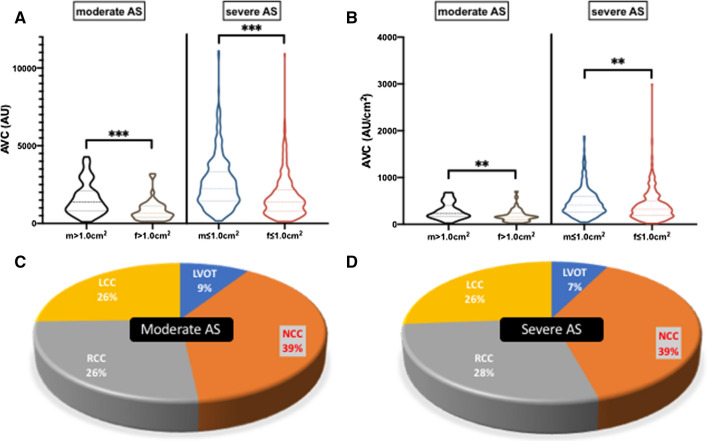
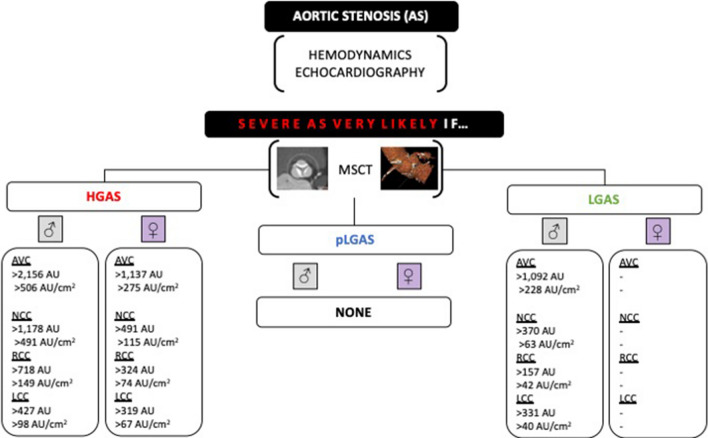
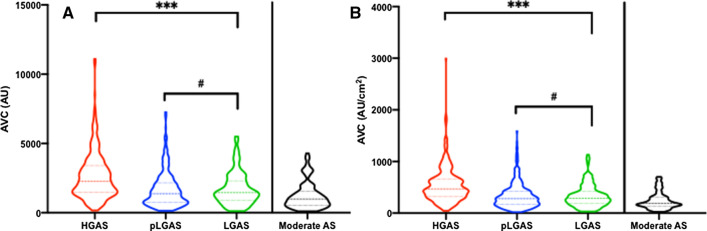
Sex- and flow-related aortic valve calcification (AVC) studies are still limited in number, and data on the exact calcium quantity and distribution are scarce. Therefore, we aimed to (1) re-define the best threshold of AVC load to distinguish severe from moderate aortic stenosis (AS) in common AS entities and to (2) evaluate differences in the aortic annulus and left ventricular outflow tract (LVOT) calcium load. Nine hundred and thirty-eight patients with contrast-enhanced cardiac MSCT and moderate-to-severe aortic stenosis (AS) were retrospectively enrolled. Patients with severe AS ≤ 1.0 cm (n = 841) were further separated into three AS entities: high gradient (HGAS, n = 370, 44.0%), paradoxical low gradient (pLGAS, n = 333, 39.6%), and classical low gradient (LGAS, n = 138, 16.4%). AVC, leaflet, and LVOT calcification were quantified. Aortic valve calcification scores were highest in severe HGAS, and lower in severe pLGAS and classical LGAS. In all severity and AS entities, the non-coronary cusp (NCC) was the most calcified one. LVOT calcification was consistently comparable between gender and AS entities. Accuracy of logistic regression was the highest in HGAS (male vs. female: AVC > 2156 Agatston units (AU), c-index 0.76; vs. AVC > 1292 AU, c-index 0.85; or AVC density > 406 AU/cm, c-index 0.82; vs. > 259 AU/cm, c-index 0.86; each p < 0.0001*) to diagnose severe AS. AVC could only be used in men to differentiate between severe LGAS and moderate AS. Data from this retrospective analysis indicate that the NCC is subject to pre-dominant degeneration throughout gender, AS severity, and several AS entities. AVC was consistently comparable in severe pLGAS and classical LGAS, but only AVC in severe LGAS could sufficiently distinguish from moderate AS in men. LVOT calcification failed to be a reliable indicator of accelerating AS.
主动脉瓣钙化(AVC)的性别和血流相关研究仍然数量有限,关于确切钙量和分布的数据也很缺乏。因此,我们的目的是:(1)重新定义 AVC 负荷的最佳阈值,以区分常见 AS 实体中的重度和中度主动脉瓣狭窄(AS);(2)评估主动脉瓣环和左心室流出道(LVOT)钙负荷的差异。我们回顾性地纳入了 938 名接受对比增强型心脏 MSCT 检查且患有中度至重度 AS 的患者。进一步将重度 AS ≤1.0cm 的患者(n=841)分为三种 AS 实体:高梯度(HGAS,n=370,44.0%)、反常低梯度(pLGAS,n=333,39.6%)和经典低梯度(LGAS,n=138,16.4%)。定量评估了 AVC、瓣叶和 LVOT 钙化情况。在所有严重程度和 AS 实体中,非冠状动脉瓣(NCC)钙化最严重。在所有严重程度和 AS 实体中,LVOT 钙化在性别和 AS 实体之间始终具有可比性。在 HGAS 中,逻辑回归的准确性最高(男性与女性相比:AVC>2156Agatston 单位(AU)时,c 指数为 0.76;AVC>1292AU 时,c 指数为 0.85;或 AVC 密度>406AU/cm 时,c 指数为 0.82;>259AU/cm 时,c 指数为 0.86;p<0.0001*),可用于诊断重度 AS。AVC 仅可用于男性,以区分重度 LGAS 和中度 AS。本回顾性分析的数据表明,NCC 在性别、AS 严重程度和几种 AS 实体中均存在主导性退变。重度 pLGAS 和经典 LGAS 之间的 AVC 始终具有可比性,但只有男性重度 LGAS 中的 AVC 才能与中度 AS 充分区分。LVOT 钙化未能成为加速 AS 的可靠指标。