Nierer Lukas, Walter Franziska, Niyazi Maximilian, Shpani Roel, Landry Guillaume, Marschner Sebastian, von Bestenbostel Rieke, Dinkel Dominika, Essenbach Gabriela, Reiner Michael, Belka Claus, Corradini Stefanie
Department of Radiation Oncology, University Hospital, LMU Munich, Marchioninistr. 15, 81377, Munich, Germany.
Radiat Oncol. 2020 Sep 10;15(1):215. doi: 10.1186/s13014-020-01657-6.
To report on our clinical experience with a newly implemented workflow for radiotherapy (RT) emergency treatments, which allows for a fast treatment application outside the regular working-hours, and its clinical applicability.
Treatment planning of 18 emergency RT patients was carried out using diagnostic computed tomography (CT) without a dedicated RT simulation CT. The cone-beam CT (CBCT) deviations of the first RT treatment were analyzed regarding setup accuracy. Furthermore, feasibility of the "fast-track" workflow was evaluated with respect to dose deviations caused by different Hounsfield unit (HU) to relative electron density (rED) calibrations and RT treatment couch surface shapes via 3D gamma index analysis of exemplary treatment plans. The dosimetric uncertainty introduced by different CT calibrations was quantified.
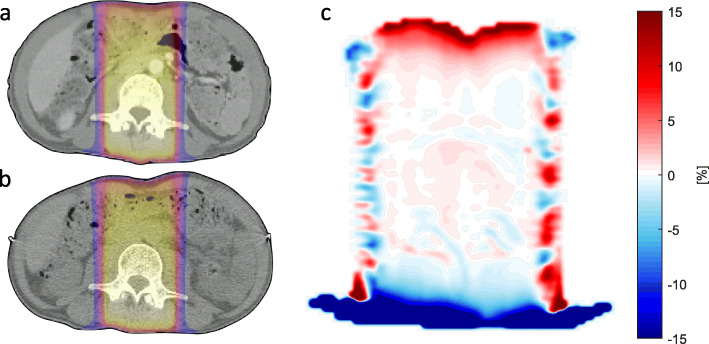
Mean patient setup vs. CBCT isocenter deviations were (0.49 ± 0.44) cm (x), (2.68 ± 1.63) cm (y) and (1.80 ± 1.06) cm (z) for lateral, longitudinal and vertical directions, respectively. Three out of four dose comparisons between the emergency RT plan calculated on the diagnostic CT and the same plan calculated on the treatment planning CT showed clinically acceptable gamma passing rates, when correcting for surface artifacts. The maximum difference of rED was 0.054, while most parts of the CT calibration curves coincided well.
In an emergency RT setting, the use of diagnostic CT data for treatment planning might be time-saving and was shown to be suitable for many cases, considering reproducibility of patient setup, accuracy of initial patient setup and accuracy of dose-calculation.
报告我们新实施的放射治疗(RT)紧急治疗工作流程的临床经验,该流程允许在正常工作时间之外快速进行治疗,并探讨其临床适用性。
对18例紧急RT患者进行治疗计划,使用诊断计算机断层扫描(CT),而非专用的RT模拟CT。分析首次RT治疗时锥形束CT(CBCT)的偏差,以评估摆位精度。此外,通过对示例性治疗计划进行三维伽马指数分析,评估“快速通道”工作流程在不同亨氏单位(HU)到相对电子密度(rED)校准以及RT治疗床表面形状导致的剂量偏差方面的可行性。量化不同CT校准引入的剂量学不确定性。
患者摆位与CBCT等中心的平均偏差在横向、纵向和垂直方向分别为(0.49±0.44)cm(x)、(2.68±1.63)cm(y)和(1.80±1.06)cm(z)。在对诊断CT上计算的紧急RT计划与治疗计划CT上计算的相同计划进行的四次剂量比较中,有三次在校正表面伪影后显示出临床可接受的伽马通过率。rED的最大差异为0.054,而CT校准曲线的大部分部分吻合良好。
在紧急RT情况下,使用诊断CT数据进行治疗计划可能节省时间,并且从患者摆位的可重复性、初始患者摆位的准确性和剂量计算的准确性来看,适用于许多病例。