Division of Internal Medicine, Rutgers Robert Wood Johnson Medical School/Saint Peter's University Hospital, New Brunswick, New Jersey.
Am J Trop Med Hyg. 2020 Nov;103(5):1989-1992. doi: 10.4269/ajtmh.20-0869.
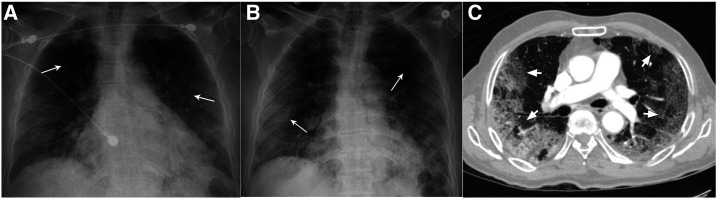
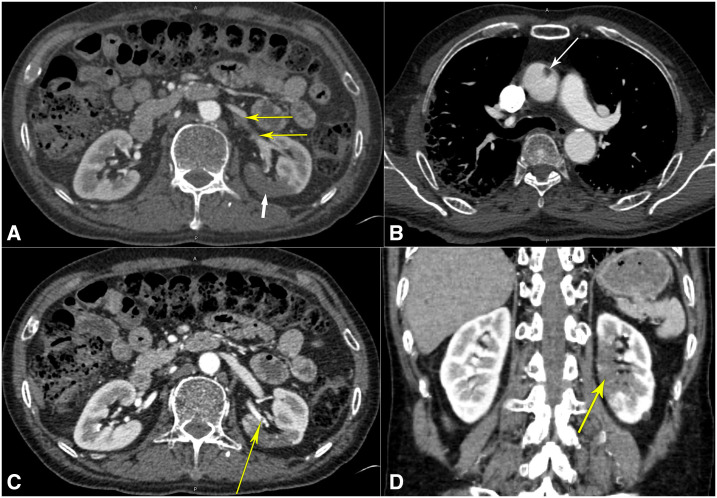
Following its discovery in Wuhan, China, in December 2019, COVID-19 has attained pandemic status in mere months. It is caused by SARS-CoV-2, an enveloped beta coronavirus. This infection causes a prothrombogenic state by interplay of inflammatory mediators, and endothelial, microvascular, and possible hepatic damage and tissue tropism of the virus. This leads to frequent pulmonary and cerebral thromboembolism as well as occasional involvement of other organs. We present a 71-year-old man who initially presented with 2 weeks of fever, cough, and shortness of breath and was diagnosed with COVID-19 pneumonia. He required readmission due to worsened hypoxia and was later found to have left renal artery thrombosis with left kidney infarction, associated with an ascending aortic thrombus. He was anticoagulated and recovered uneventfully. We suggest that physicians have a high degree of suspicion to diagnose and manage the novel manifestations of this disease.
自 2019 年 12 月在中国武汉发现以来,COVID-19 在短短几个月内就达到了大流行的程度。它是由 SARS-CoV-2 引起的,一种包膜的β冠状病毒。这种感染通过炎症介质的相互作用,以及内皮、微血管和可能的肝损伤和病毒的组织嗜性,导致促血栓形成状态。这导致经常发生肺和脑血栓栓塞,偶尔也会涉及其他器官。我们介绍了一名 71 岁男性,他最初表现为发热、咳嗽和呼吸急促,并被诊断为 COVID-19 肺炎。由于缺氧恶化,他需要再次入院治疗,后来发现他患有左肾动脉血栓形成和左肾梗死,伴有升主动脉血栓。他接受了抗凝治疗,恢复顺利。我们建议医生高度怀疑诊断和管理这种疾病的新表现。