Dambha-Miller Hajira, Albasri Ali, Hodgson Sam, Wilcox Christopher R, Khan Shareen, Islam Nazrul, Little Paul, Griffin Simon J
Department of Primary Care, University of Southampton, Southampton, UK
MRC Epidemiology Unit, University of Cambridge, Cambridge, UK.
BMJ Open. 2020 Sep 14;10(9):e040644. doi: 10.1136/bmjopen-2020-040644.
To review evidence on routinely prescribed drugs in the UK that could upregulate or downregulate ACE2 and potentially affect COVID-19 disease.
Systematic review.
MEDLINE, EMBASE, CINAHL, the Cochrane Library and Web of Science.
Any design with animal or human models examining a currently prescribed UK drug compared with a control, placebo or sham group, and reporting an effect on ACE2 level, activity or gene expression.
MEDLINE, EMBASE, CINAHL, the Cochrane Library, Web of Science and OpenGrey from inception to 1 April 2020. Methodological quality was assessed using the SYstematic Review Centre for Laboratory animal Experimentation (SYRCLE) risk-of-bias tool for animal studies and Cochrane risk-of-bias tool for human studies.
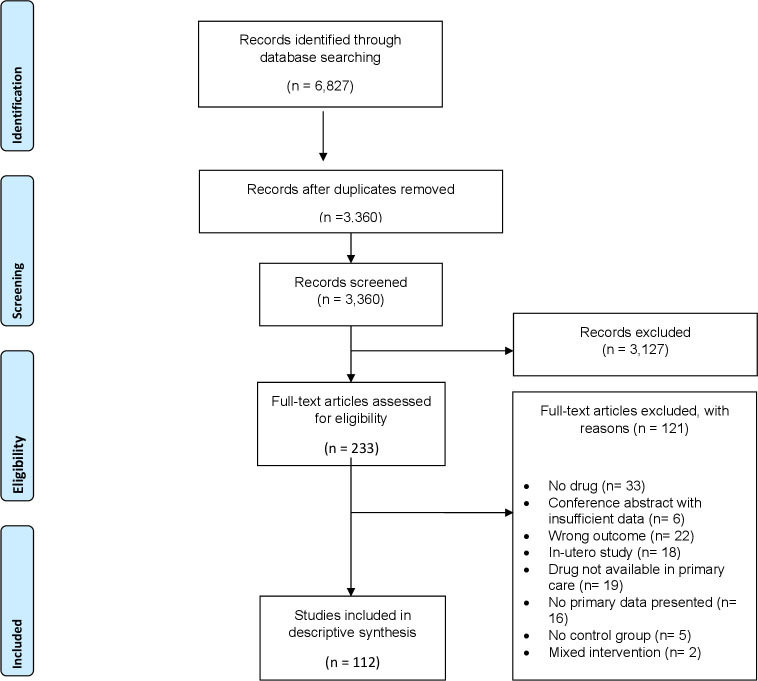
We screened 3360 titles and included 112 studies with 21 different drug classes identified as influencing ACE2 activity. Ten studies were in humans and one hundred and two were in animal models None examined ACE2 in human lungs. The most frequently examined drugs were angiotensin receptor blockers (ARBs) (n=55) and ACE inhibitors (ACE-I) (n=22). More studies reported upregulation than downregulation with ACE-I (n=22), ARBs (n=55), insulin (n=8), thiazolidinedione (n=7) aldosterone agonists (n=3), statins (n=5), oestrogens (n=5) calcium channel blockers (n=3) glucagon-like peptide 1 (GLP-1) agonists (n=2) and Non-steroidal anti-inflammatory drugs (NSAIDs) (n=2).
There is an abundance of the academic literature and media reports on the potential of drugs that could attenuate or exacerbate COVID-19 disease. This is leading to trials of repurposed drugs and uncertainty among patients and clinicians concerning continuation or cessation of prescribed medications. Our review indicates that the impact of currently prescribed drugs on ACE2 has been poorly studied in vivo, particularly in human lungs where the SARS-CoV-2 virus appears to enact its pathogenic effects. We found no convincing evidence to justify starting or stopping currently prescribed drugs to influence outcomes of COVID-19 disease.
综述英国常规处方药物中可能上调或下调血管紧张素转换酶2(ACE2)并可能影响新冠肺炎病情的相关证据。
系统评价。
医学期刊数据库(MEDLINE)、荷兰医学文摘数据库(EMBASE)、护理学与健康领域数据库(CINAHL)、考克兰图书馆及科学引文索引数据库(Web of Science)。
采用动物或人体模型的任何设计,将一种当前在英国开具的处方药与对照组、安慰剂组或假手术组进行比较,并报告对ACE2水平、活性或基因表达的影响。
检索MEDLINE、EMBASE、CINAHL、考克兰图书馆、Web of Science及OpenGrey数据库,检索时间从建库至2020年4月1日。使用实验室动物实验系统评价中心(SYRCLE)的动物研究偏倚风险工具和考克兰人类研究偏倚风险工具评估方法学质量。
我们筛选了3360篇文献,纳入112项研究,确定有21种不同药物类别可影响ACE2活性。10项研究涉及人类,102项研究涉及动物模型,均未在人肺中检测ACE2。研究最多的药物是血管紧张素受体阻滞剂(ARB)(n = 55)和血管紧张素转换酶抑制剂(ACE-I)(n = 22)。更多研究报告ACE-I(n = 22)、ARB(n = 55)、胰岛素(n = 8)、噻唑烷二酮类(n = 7)、醛固酮激动剂(n = 3)、他汀类药物(n = 5)、雌激素(n = 5)、钙通道阻滞剂(n = 3)、胰高血糖素样肽1(GLP-1)激动剂(n = 2)和非甾体抗炎药(NSAIDs)(n = 2)具有上调作用而非下调作用。
关于药物可能减轻或加重新冠肺炎病情的潜力,有大量学术文献和媒体报道。这导致了对旧药的试验,以及患者和临床医生在继续或停止使用处方药方面的不确定性。我们的综述表明,目前开具的药物对ACE2的影响在体内研究较少,尤其是在SARS-CoV-2病毒似乎发挥致病作用的人肺中。我们没有找到令人信服的证据来证明开始或停止使用目前开具的药物以影响新冠肺炎病情的转归是合理的。